Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- 2.tfs Spring Source DDocumento2 páginas2.tfs Spring Source DErica DouglasAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- E91347 PDFDocumento58 páginasE91347 PDFErica DouglasAinda não há avaliações
- WHO Hand Hygiene Community Campaign PDFDocumento2 páginasWHO Hand Hygiene Community Campaign PDFErica DouglasAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- ECE MP - WH 13 Add.2 ENG PDFDocumento28 páginasECE MP - WH 13 Add.2 ENG PDFErica DouglasAinda não há avaliações
- Ece MP - Wat 17 PDFDocumento65 páginasEce MP - Wat 17 PDFErica DouglasAinda não há avaliações
- UN Map Feb.2012 PDFDocumento1 páginaUN Map Feb.2012 PDFErica DouglasAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- INF8 Item11 ENG Equitable Access Publication Outline RevDocumento5 páginasINF8 Item11 ENG Equitable Access Publication Outline RevErica DouglasAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
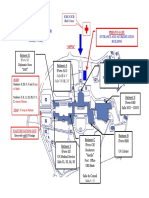
- Security Identification Sub-Unit: Open 0800 - 1700, Non-Stop Monday - Friday Entrance and Accreditation BuildingDocumento1 páginaSecurity Identification Sub-Unit: Open 0800 - 1700, Non-Stop Monday - Friday Entrance and Accreditation BuildingErica DouglasAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Environmental and Policy Cardiovascular Disease PreventionDocumento17 páginasEnvironmental and Policy Cardiovascular Disease PreventionErica DouglasAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Progress On: Drinking Water, Sanitation and HygieneDocumento116 páginasProgress On: Drinking Water, Sanitation and HygieneErica DouglasAinda não há avaliações
- Final UKHealthForum SatFatresponse241013Documento2 páginasFinal UKHealthForum SatFatresponse241013Erica DouglasAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- JMP For Water Supply and SanitationDocumento13 páginasJMP For Water Supply and SanitationErica DouglasAinda não há avaliações
- E FinalWebDocumento30 páginasE FinalWebErica DouglasAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Cho Gsas - Harvard 0084L 11462Documento503 páginasCho Gsas - Harvard 0084L 11462Claudemiro costaAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- API Casing Collapse CalcsDocumento8 páginasAPI Casing Collapse CalcsJay SadAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- 1704 Broschuere Metal-Coating en EinzelseitenDocumento8 páginas1704 Broschuere Metal-Coating en EinzelseiteninterponAinda não há avaliações
- EMV Card Reader Upgrade Kit Instructions - 05162016Documento6 páginasEMV Card Reader Upgrade Kit Instructions - 05162016Shashi K KumarAinda não há avaliações
- Air System Sizing Summary For NIVEL PB - Zona 1Documento1 páginaAir System Sizing Summary For NIVEL PB - Zona 1Roger PandoAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Feasibility Study On The Seaweed Kappaphycus Alvarezii Cultivation Site in Indari Waters ofDocumento9 páginasFeasibility Study On The Seaweed Kappaphycus Alvarezii Cultivation Site in Indari Waters ofUsman MadubunAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Pediatric Gynecology BaruDocumento79 páginasPediatric Gynecology BaruJosephine Irena100% (2)
- Medical CodingDocumento5 páginasMedical CodingBernard Paul GuintoAinda não há avaliações
- Notice - Appeal Process List of Appeal Panel (Final 12.1.24)Documento13 páginasNotice - Appeal Process List of Appeal Panel (Final 12.1.24)FyBerri InkAinda não há avaliações
- HACH LANGE Amino Acid F Reagent Powder (2353255)Documento6 páginasHACH LANGE Amino Acid F Reagent Powder (2353255)kerem__22Ainda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Plaquette - PRECASEM - CIMEC 2019 English VersionDocumento18 páginasPlaquette - PRECASEM - CIMEC 2019 English VersionFranck BertrandAinda não há avaliações
- T 1246784488 17108574 Street Lighting Control Based On LonWorks Power Line CommunicationDocumento3 páginasT 1246784488 17108574 Street Lighting Control Based On LonWorks Power Line CommunicationsryogaaAinda não há avaliações
- Strange Christmas TraditionsDocumento2 páginasStrange Christmas TraditionsZsofia ZsofiaAinda não há avaliações
- Theory of Earth's Magnetism and It's Relation ToDocumento15 páginasTheory of Earth's Magnetism and It's Relation ToMaster Irvin100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Inverse Curve Trip Time Calculation: Enter Values in White CellDocumento3 páginasInverse Curve Trip Time Calculation: Enter Values in White CellVijay FxAinda não há avaliações
- Solids Separation Study Guide: Wisconsin Department of Natural Resources Wastewater Operator CertificationDocumento44 páginasSolids Separation Study Guide: Wisconsin Department of Natural Resources Wastewater Operator CertificationkharismaaakAinda não há avaliações
- Case Study (Co2 Flooding)Documento10 páginasCase Study (Co2 Flooding)Jessica KingAinda não há avaliações
- Ield Methods: A Typical Field Mapping Camp in The 1950sDocumento4 páginasIeld Methods: A Typical Field Mapping Camp in The 1950sshivam soniAinda não há avaliações
- Commercial Kitchen Fire InvestigationsDocumento6 páginasCommercial Kitchen Fire InvestigationsBen ConnonAinda não há avaliações
- Hyundai Forklift Catalog PTASDocumento15 páginasHyundai Forklift Catalog PTASjack comboAinda não há avaliações
- Charles Haanel - The Master Key System Cd2 Id1919810777 Size878Documento214 páginasCharles Haanel - The Master Key System Cd2 Id1919810777 Size878Hmt Nmsl100% (2)
- Biochem Acids and Bases Lab ReportDocumento4 páginasBiochem Acids and Bases Lab ReportShaina MabborangAinda não há avaliações
- Equipment in The NICUDocumento7 páginasEquipment in The NICUGheDine PeracionAinda não há avaliações
- Boyle's Law 2023Documento6 páginasBoyle's Law 2023Justin HuynhAinda não há avaliações
- Rezhna Hassan FarajDocumento2 páginasRezhna Hassan FarajchristoptAinda não há avaliações
- Smith KJ Student Mathematics Handbook and Integral Table ForDocumento328 páginasSmith KJ Student Mathematics Handbook and Integral Table ForStrahinja DonicAinda não há avaliações
- Brainedema 160314142234Documento39 páginasBrainedema 160314142234Lulu LuwiiAinda não há avaliações
- Barium SulphateDocumento11 páginasBarium SulphateGovindanayagi PattabiramanAinda não há avaliações
- Goal 6 Unesco Water SanatationDocumento5 páginasGoal 6 Unesco Water Sanatationapi-644347009Ainda não há avaliações