Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Court Document SummaryDocumento15 páginasCourt Document SummaryAkAsh prAkhAr vErmA100% (1)
- Worksheet Pirates of The Caribbean Curse of TheDocumento3 páginasWorksheet Pirates of The Caribbean Curse of TheAylin Acar0% (1)
- 2.arteri Complication PVDocumento5 páginas2.arteri Complication PVNovi Yanti NyAinda não há avaliações
- 148E CPG August2004Documento7 páginas148E CPG August2004Ekhlas Al-AbsyAinda não há avaliações
- A Case of Uncorrected Tetralogy of Fallot Undiagnosed Presenting With Polycythemia On Rural Area in South-East Asia SettingDocumento5 páginasA Case of Uncorrected Tetralogy of Fallot Undiagnosed Presenting With Polycythemia On Rural Area in South-East Asia SettingNovi Yanti NyAinda não há avaliações
- 2020 ESC Guidelines For The Management of Adult Congenital Heart Disease (Previously Grown-Up Congenital Heart Disease)Documento84 páginas2020 ESC Guidelines For The Management of Adult Congenital Heart Disease (Previously Grown-Up Congenital Heart Disease)Liliana BrochadoAinda não há avaliações
- Kesimpulan Dan Saran PancasilaDocumento21 páginasKesimpulan Dan Saran PancasilaNovi Yanti NyAinda não há avaliações
- Daftar Pustaka Journal ReadingDocumento4 páginasDaftar Pustaka Journal ReadingNovi Yanti NyAinda não há avaliações
- DengueDocumento38 páginasDenguevoruganty_vvsAinda não há avaliações
- J Jclinane 2005 08 012Documento3 páginasJ Jclinane 2005 08 012Novi Yanti NyAinda não há avaliações
- Digital Hypertension PowerPoint Templates StandardDocumento3 páginasDigital Hypertension PowerPoint Templates StandardPuskesmas Purwokerto SelatanAinda não há avaliações
- Guidelines For The Treatment of Drug-Susceptible Tuberculosis (TB) and Patient Care 2017 PDFDocumento80 páginasGuidelines For The Treatment of Drug-Susceptible Tuberculosis (TB) and Patient Care 2017 PDFILa' ArmiLa LomatAinda não há avaliações
- 2014 ESC/ESA Guidelines On Non-Cardiac Surgery: Cardiovascular Assessment and ManagementDocumento49 páginas2014 ESC/ESA Guidelines On Non-Cardiac Surgery: Cardiovascular Assessment and ManagementNovi Yanti NyAinda não há avaliações
- 2 PB - 2 PDFDocumento6 páginas2 PB - 2 PDFMuh Fajar Eka PutraAinda não há avaliações
- Jurnal DM 08 PDFDocumento11 páginasJurnal DM 08 PDFNovi Yanti NyAinda não há avaliações
- Eappendix A. Guideline Summary For Preoperative EcgDocumento7 páginasEappendix A. Guideline Summary For Preoperative EcgNovi Yanti NyAinda não há avaliações
- 2019 Medical Plan PowerPoint TemplatesDocumento48 páginas2019 Medical Plan PowerPoint TemplatesAnonymous 0XjTzZf1f100% (1)
- Galveston Orientation Amnesia Test PDFDocumento1 páginaGalveston Orientation Amnesia Test PDFsyahbian100% (1)
- 2 PB - 2 PDFDocumento6 páginas2 PB - 2 PDFMuh Fajar Eka PutraAinda não há avaliações
- Penelitian Tentang Penyakit JantungDocumento1 páginaPenelitian Tentang Penyakit Jantungvhiga gionataAinda não há avaliações
- 148E CPG August2004Documento7 páginas148E CPG August2004Ekhlas Al-AbsyAinda não há avaliações
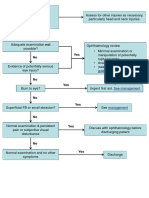
- No Yes: Penetrating Eye Injury GuidelinesDocumento1 páginaNo Yes: Penetrating Eye Injury GuidelinesNovi Yanti NyAinda não há avaliações
- Hypertensionin PregnancyDocumento100 páginasHypertensionin Pregnancyricky hutagalungAinda não há avaliações
- Hallmarks of Cancer: The Next GenerationDocumento29 páginasHallmarks of Cancer: The Next GenerationAllanM.SchiffmanAinda não há avaliações
- Cutaneous Manifestations in HIV Positive Paediatric PatientsDocumento6 páginasCutaneous Manifestations in HIV Positive Paediatric PatientsNovi Yanti NyAinda não há avaliações
- 1071 FullDocumento3 páginas1071 FullNovi Yanti NyAinda não há avaliações
- Forensic Toxicological Analysis in Cyanide Poisoning Two Case ReportsDocumento32 páginasForensic Toxicological Analysis in Cyanide Poisoning Two Case ReportsNovi Yanti NyAinda não há avaliações
- Altered Cardiovascular Variability in Obstructive Sleep ApneaDocumento8 páginasAltered Cardiovascular Variability in Obstructive Sleep ApneaNovi Yanti NyAinda não há avaliações
- Altered Cardiovascular Variability in Obstructive Sleep ApneaDocumento8 páginasAltered Cardiovascular Variability in Obstructive Sleep ApneaNovi Yanti NyAinda não há avaliações
- Forensic Toxicological Analysis in Cyanide Poisoning Two Case ReportsDocumento3 páginasForensic Toxicological Analysis in Cyanide Poisoning Two Case ReportsNovi Yanti NyAinda não há avaliações
- Forensic Toxicological Analysis in Cyanide Poisoning Two Case ReportsDocumento32 páginasForensic Toxicological Analysis in Cyanide Poisoning Two Case ReportsNovi Yanti NyAinda não há avaliações
- Important Tips On The Law On SalesDocumento34 páginasImportant Tips On The Law On SalesJanetGraceDalisayFabreroAinda não há avaliações
- The Transformation of PhysicsDocumento10 páginasThe Transformation of PhysicsVíctor Manuel Hernández MárquezAinda não há avaliações
- Semaphore Twinsoft Manual PDFDocumento101 páginasSemaphore Twinsoft Manual PDFReza AnantoAinda não há avaliações
- LAB 2 SimulationDocumento6 páginasLAB 2 SimulationArti Stic100% (1)
- Work Breakdown StructureDocumento3 páginasWork Breakdown StructureEllie Annelle LazaroAinda não há avaliações
- Biosimilars: Pros and Cons in Current Practice: MBBS, MRCP (Uk), FRCP (Edin), FamsDocumento51 páginasBiosimilars: Pros and Cons in Current Practice: MBBS, MRCP (Uk), FRCP (Edin), FamshoneyworksAinda não há avaliações
- Assessment - The Bridge Between Teaching and Learning (VFTM 2013)Documento6 páginasAssessment - The Bridge Between Teaching and Learning (VFTM 2013)Luis CYAinda não há avaliações
- Vastu Colors (Room by Room Home Coloring Guide)Documento25 páginasVastu Colors (Room by Room Home Coloring Guide)yuva razAinda não há avaliações
- BSD Magazine MaioDocumento101 páginasBSD Magazine MaioBruno AlvimAinda não há avaliações
- Greenbelt Place ApartmentsDocumento8 páginasGreenbelt Place ApartmentsTricia EnnisAinda não há avaliações
- PrisonerDocumento10 páginasPrisonerAbdi ShakourAinda não há avaliações
- Casalla vs. PeopleDocumento2 páginasCasalla vs. PeopleJoan Eunise FernandezAinda não há avaliações
- Field Study 2 Ep. 5 AnswerDocumento10 páginasField Study 2 Ep. 5 AnswerShane Via CainticAinda não há avaliações
- Chisholm - Referring To Things That No Longer ExistDocumento13 páginasChisholm - Referring To Things That No Longer ExistMichele Paolini PaolettiAinda não há avaliações
- Homemade Water PurifierDocumento13 páginasHomemade Water PurifierSherazAinda não há avaliações
- DocxDocumento2 páginasDocxNashAinda não há avaliações
- ECO 201 Sample Midterm Exam (Paulo GuimaraesDocumento14 páginasECO 201 Sample Midterm Exam (Paulo GuimaraesAhmed NegmAinda não há avaliações
- What Is Six Sigma: Everything You Need To Know About It: by Pankaj KumarDocumento16 páginasWhat Is Six Sigma: Everything You Need To Know About It: by Pankaj KumarSuman DewanAinda não há avaliações
- Aprils Detox GuideDocumento20 páginasAprils Detox GuideKwasi BempongAinda não há avaliações
- Matrix Software User ManuelDocumento45 páginasMatrix Software User ManuelHema SantoshAinda não há avaliações
- Assessing Learning Methods and TestsDocumento2 páginasAssessing Learning Methods and TestsZarah Joyce SegoviaAinda não há avaliações
- What Is Link AdaptationDocumento4 páginasWhat Is Link AdaptationAshutosh SinghAinda não há avaliações
- KNAW Proceedings from 1919-1920Documento481 páginasKNAW Proceedings from 1919-1920Eduardo Salgado EnríquezAinda não há avaliações
- TO B.inggris Dzakiy Bag 2Documento21 páginasTO B.inggris Dzakiy Bag 2Ayu RatnaAinda não há avaliações
- Application for Test Engineer PositionDocumento3 páginasApplication for Test Engineer PositionAsz WaNieAinda não há avaliações
- Paper - Iii Law of Torts (Paper Code: K-103) : Books RecommendedDocumento1 páginaPaper - Iii Law of Torts (Paper Code: K-103) : Books Recommendedvivek6593Ainda não há avaliações