Você também pode gostar
- Green Playful Rare Animals in The World PresentationDocumento14 páginasGreen Playful Rare Animals in The World PresentationLaura Ortiz BermudezAinda não há avaliações
- Blockposter 133852Documento10 páginasBlockposter 133852Laura Ortiz BermudezAinda não há avaliações
- Wip PascuaDocumento6 páginasWip PascuaLaura Ortiz BermudezAinda não há avaliações
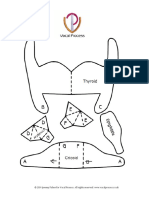
- Build Your Own Tilting Larynx From PaperDocumento2 páginasBuild Your Own Tilting Larynx From PaperPaula BinnieAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Zoderm e CreamDocumento5 páginasZoderm e CreamUmesh ShengalAinda não há avaliações
- Classical Homoeopathy Book FourDocumento99 páginasClassical Homoeopathy Book FourYaniv Algrably100% (1)
- Introduction To Clinical Psychology Notes 1Documento83 páginasIntroduction To Clinical Psychology Notes 1Paulo Miguel GernaleAinda não há avaliações
- Mechanism of AB ResistanceDocumento31 páginasMechanism of AB ResistancesarasatiwanamiAinda não há avaliações
- Experience of Dental Caries in Mother/child Pairs: Association Between Risk Indicators and Dental CariesDocumento8 páginasExperience of Dental Caries in Mother/child Pairs: Association Between Risk Indicators and Dental CariesRisky Anita OktavianiAinda não há avaliações
- ID Regulasi Keamanan Hayati Produk Rekayasa PDFDocumento18 páginasID Regulasi Keamanan Hayati Produk Rekayasa PDFPangihutan manaluAinda não há avaliações
- Brenner and Rector's The Kidney, 2-Volume Set, 10th Edition: Skorecki, Chertow, Marsden, Taal & YuDocumento4 páginasBrenner and Rector's The Kidney, 2-Volume Set, 10th Edition: Skorecki, Chertow, Marsden, Taal & YuJim Dominguez RosalesAinda não há avaliações
- Comprehensive Pharmacy Review SummaryDocumento143 páginasComprehensive Pharmacy Review SummaryjaninamariesarmientoAinda não há avaliações
- Biologic Width - The No Encroachment Zone: I J D ADocumento8 páginasBiologic Width - The No Encroachment Zone: I J D AJinny ShawAinda não há avaliações
- Influencia de La Postura Del Pie en El Mecanismo de Windlass, Ensayo ClinicoDocumento20 páginasInfluencia de La Postura Del Pie en El Mecanismo de Windlass, Ensayo ClinicoAlberto Jesús CamposAinda não há avaliações
- Msds Jotafloor Topcoat Comp ADocumento6 páginasMsds Jotafloor Topcoat Comp AzayzanAinda não há avaliações
- Malta Driving StandardsDocumento6 páginasMalta Driving StandardsAnne Marie ScerriAinda não há avaliações
- Emergency Management of Severe BurnsDocumento97 páginasEmergency Management of Severe BurnsAyu SyartikaAinda não há avaliações
- Phonetics in Complete Denture-3670Documento5 páginasPhonetics in Complete Denture-3670Najeeb UllahAinda não há avaliações
- StatSensor Creatinine Brochure - CDN vs.177Documento8 páginasStatSensor Creatinine Brochure - CDN vs.177Eva Nada MaulidaAinda não há avaliações
- Otc Drug Drug InteractionsDocumento3 páginasOtc Drug Drug InteractionsDavid HosamAinda não há avaliações
- 50 Millesimal Potency Intheory and Practice Harimohon Choudhury.00012 - 2contentsDocumento5 páginas50 Millesimal Potency Intheory and Practice Harimohon Choudhury.00012 - 2contentsMd. NazimAinda não há avaliações
- Table of Differentiation of ParasitesDocumento18 páginasTable of Differentiation of ParasitesManuel RendonAinda não há avaliações
- Aparna FinalDocumento59 páginasAparna FinalPraveen PuthuparambilAinda não há avaliações
- Non-Communicable Diseases - Kuntaraf Script Online VersionDocumento13 páginasNon-Communicable Diseases - Kuntaraf Script Online VersionSadiki WallaceAinda não há avaliações
- General Anxiety Remedies in HomeopathyDocumento5 páginasGeneral Anxiety Remedies in Homeopathyvijay kumarAinda não há avaliações
- NothingNewUnderTheSun Abdul HamidHughesDocumento10 páginasNothingNewUnderTheSun Abdul HamidHughesLuisdaniel Martinez AranaAinda não há avaliações
- Pa Tho Physiology of Angina PectorisDocumento2 páginasPa Tho Physiology of Angina PectorisChristine Elaine Batusin IlaganAinda não há avaliações
- Tanda - Tanda VitalDocumento4 páginasTanda - Tanda VitalImelda ChristinaAinda não há avaliações
- Drug of ChoiceDocumento4 páginasDrug of ChoiceJohnmark DubdubanAinda não há avaliações
- Sandeep MedicalDocumento2 páginasSandeep MedicalSandeep GAMING YTAinda não há avaliações
- Intradialytic Hypotension: Arwedi ArwantoDocumento17 páginasIntradialytic Hypotension: Arwedi ArwantopiusiAinda não há avaliações
- Psychoactive Plants Tobacco, Peyote, Kava, and Other PlantsDocumento5 páginasPsychoactive Plants Tobacco, Peyote, Kava, and Other PlantstysonAinda não há avaliações
- FEB Brickclean Safety DatasheetDocumento10 páginasFEB Brickclean Safety DatasheetMhd ThrAinda não há avaliações
- CL November2016Documento24 páginasCL November2016patruoxAinda não há avaliações