Você também pode gostar
- MSDC 5555Documento11 páginasMSDC 5555John M. Hemsworth100% (1)
- Spinal Segmental Sensitization As A Common OriginDocumento8 páginasSpinal Segmental Sensitization As A Common OriginRossangel Huapaya RomeroAinda não há avaliações
- Injuries Complicating Musical Practice A PDFDocumento4 páginasInjuries Complicating Musical Practice A PDFFerrari En ZoAinda não há avaliações
- Advances in The Diagnosis & Management of Neck Pain - Article.Documento19 páginasAdvances in The Diagnosis & Management of Neck Pain - Article.salmankhan09215Ainda não há avaliações
- Management L Low Back PainDocumento7 páginasManagement L Low Back PainelsyamelindaAinda não há avaliações
- Biochemistry Lab Module 2 Case 2 #1,2Documento3 páginasBiochemistry Lab Module 2 Case 2 #1,2theodore_estradaAinda não há avaliações
- FDAR (Sample)Documento3 páginasFDAR (Sample)Zarah Joy Tabuyan88% (17)
- Head and Neck and Endocrine Surgery From Clinical Presentation To Treatment Success 1st Ed 2016Documento400 páginasHead and Neck and Endocrine Surgery From Clinical Presentation To Treatment Success 1st Ed 2016Luan MatosAinda não há avaliações
- Takagiryu HistoryDocumento10 páginasTakagiryu HistoryTerry LollbackAinda não há avaliações
- Leadership and Management For NursesDocumento18 páginasLeadership and Management For NursesmerAinda não há avaliações
- Check List For AmbulanceDocumento2 páginasCheck List For AmbulanceEka B100% (1)
- 8th TNM Clasification - Lung CancerDocumento10 páginas8th TNM Clasification - Lung CancerEma ȚurcașAinda não há avaliações
- Business Plan For 100 Bedeed HospitalDocumento36 páginasBusiness Plan For 100 Bedeed HospitalsbhatiAinda não há avaliações
- Tegner Lysholm Knee Scoring Scale - Orthopaedic ScoresDocumento2 páginasTegner Lysholm Knee Scoring Scale - Orthopaedic Scoresradu_pavalache100% (2)
- Anecdotal RecordsDocumento21 páginasAnecdotal RecordsShubhrima Khan100% (1)
- Respiratory Failure in Children PDFDocumento47 páginasRespiratory Failure in Children PDFOxana TurcuAinda não há avaliações
- Traumatic Neuralgia From Pressure-Point Strikes in The Martial Arts - Results From A Retrospective Online SurveyDocumento4 páginasTraumatic Neuralgia From Pressure-Point Strikes in The Martial Arts - Results From A Retrospective Online Survey_craven_Ainda não há avaliações
- Injuries - Complicating - Musical - Practice - A20160908 13997 Qigc42 With Cover Page v2 1Documento5 páginasInjuries - Complicating - Musical - Practice - A20160908 13997 Qigc42 With Cover Page v2 1Fábio Mota100% (1)
- Return To Play Following Muscle StrainsDocumento6 páginasReturn To Play Following Muscle StrainsSamuel Iñiguez JiménezAinda não há avaliações
- CTDs JurnalDocumento4 páginasCTDs JurnalAYU OKTAMARISKA PUTRIAinda não há avaliações
- GOOD - Muscle CrampsDocumento12 páginasGOOD - Muscle CrampsSylvia GraceAinda não há avaliações
- Axillary Nerve Palsy and Deltoid Muscle AtonyDocumento12 páginasAxillary Nerve Palsy and Deltoid Muscle AtonyLaura CandussiAinda não há avaliações
- Leddy Lambert Ogles 1994Documento9 páginasLeddy Lambert Ogles 1994Chuk DiogoAinda não há avaliações
- Handandwristinjuriesin Boxingandthemartial Arts: Benjamin Todd Drury,, Thomas P. Lehman,, Ghazi RayanDocumento10 páginasHandandwristinjuriesin Boxingandthemartial Arts: Benjamin Todd Drury,, Thomas P. Lehman,, Ghazi RayanVictor Manuel Zamora GasgaAinda não há avaliações
- Sports Medicine Meets Musculoskeletal MeDocumento3 páginasSports Medicine Meets Musculoskeletal MeMotea IoanaAinda não há avaliações
- The Ability of Clinical Tests To Diagnose Stress Fractures: A Systematic Review and Meta-AnalysisDocumento13 páginasThe Ability of Clinical Tests To Diagnose Stress Fractures: A Systematic Review and Meta-Analysischan kyoAinda não há avaliações
- Fneur 14 1104817Documento6 páginasFneur 14 1104817geowalker7092Ainda não há avaliações
- Potential Role of Stem Cells For Neuropathic Pain DisordersDocumento5 páginasPotential Role of Stem Cells For Neuropathic Pain Disordersmatheus derocoAinda não há avaliações
- Odg Seminarski Rad 2Documento10 páginasOdg Seminarski Rad 2Ivana VujisicAinda não há avaliações
- 00002.pdf JsessionidDocumento8 páginas00002.pdf JsessionidSeti Aji HAinda não há avaliações
- Jamaneurology Mckee 2023 Oi 230060 1692885331.06589Documento13 páginasJamaneurology Mckee 2023 Oi 230060 1692885331.06589yennyAinda não há avaliações
- Myofascial Trigger Points: The Current Evidence: Leesa K. HugueninDocumento11 páginasMyofascial Trigger Points: The Current Evidence: Leesa K. HugueninRo KohnAinda não há avaliações
- Advances in The Diagnosis and Management of Neck PainDocumento19 páginasAdvances in The Diagnosis and Management of Neck PainJose Fernando DiezAinda não há avaliações
- Spinal Cord Injuries Principles and MethodsDocumento26 páginasSpinal Cord Injuries Principles and MethodsBianca SantanaAinda não há avaliações
- Neurophysiology of Pain - Insight To Orofacial Pain PDFDocumento23 páginasNeurophysiology of Pain - Insight To Orofacial Pain PDFSandeep Kumar PanigrahiAinda não há avaliações
- HHS Public Access: Demystifying Post-Stroke Pain: From Etiology To TreatmentDocumento21 páginasHHS Public Access: Demystifying Post-Stroke Pain: From Etiology To TreatmentMartha OktaviaAinda não há avaliações
- Imágenes de RM de Trauma MuscularDocumento23 páginasImágenes de RM de Trauma Muscularmicamart.94Ainda não há avaliações
- Lesão Isquiotibiais Metodos e Exercícios de Recuperação - Métodos de DiagnósticoDocumento15 páginasLesão Isquiotibiais Metodos e Exercícios de Recuperação - Métodos de DiagnósticojoaoaesfigueiredoAinda não há avaliações
- Axillary Nerve PalsyDocumento11 páginasAxillary Nerve Palsyksaurabh027Ainda não há avaliações
- Neuropsychiatric Illnesses in War Veterans: Charles W. HogeDocumento6 páginasNeuropsychiatric Illnesses in War Veterans: Charles W. HogeSavanth krishna TAinda não há avaliações
- Nerve Entrapment - UpdateDocumento17 páginasNerve Entrapment - UpdatealobrienAinda não há avaliações
- Neuropathic Pain A Maladaptive Response of The NerDocumento34 páginasNeuropathic Pain A Maladaptive Response of The NerMayAinda não há avaliações
- International Spinal Cord Injury Pain Classification: Part I. Background and DescriptionDocumento5 páginasInternational Spinal Cord Injury Pain Classification: Part I. Background and DescriptionAyat BissAinda não há avaliações
- HTTPS:WWW Ncbi NLM Nih gov:pmc:articles:PMC9144471:pdf:jpm-12-00808Documento12 páginasHTTPS:WWW Ncbi NLM Nih gov:pmc:articles:PMC9144471:pdf:jpm-12-00808Ihsanul Ma'arifAinda não há avaliações
- General Principles of NeurologyDocumento8 páginasGeneral Principles of NeurologyCARZ 42Ainda não há avaliações
- Trauma: Radial Nerve PalsyDocumento9 páginasTrauma: Radial Nerve PalsyKristina DewiAinda não há avaliações
- 2018 Article 633Documento19 páginas2018 Article 633ZmajAinda não há avaliações
- Pain After SCIDocumento20 páginasPain After SCIanjelikaAinda não há avaliações
- Athletic Injuries of The ThoracicDocumento20 páginasAthletic Injuries of The ThoracicGrado CristianAinda não há avaliações
- OrthopaediDocumento12 páginasOrthopaediefancoolhand09Ainda não há avaliações
- Dor NeuropaticaDocumento4 páginasDor NeuropaticaRoderley ReisAinda não há avaliações
- Central Mechanisms of Pathological PainDocumento9 páginasCentral Mechanisms of Pathological PainRocio DominguezAinda não há avaliações
- Sonographic Diagnosis of Nontraumatic Musculotendinous Rupture of Hamstring 2008 Journal of Medical UltrasoundDocumento4 páginasSonographic Diagnosis of Nontraumatic Musculotendinous Rupture of Hamstring 2008 Journal of Medical UltrasoundIman Ru-ancaAinda não há avaliações
- Pain Coping Styles of Ballet PerformersDocumento15 páginasPain Coping Styles of Ballet PerformersNature M.Ainda não há avaliações
- Consenso de MunichDocumento10 páginasConsenso de MunichBartholomew AllenAinda não há avaliações
- Robinson 2000Documento11 páginasRobinson 2000DurgareddyAinda não há avaliações
- Thopaedic Science: JournalDocumento16 páginasThopaedic Science: JournalCiro Madrid FloresAinda não há avaliações
- Jurnal 2Documento13 páginasJurnal 2Rachmat Ratri AnggoroAinda não há avaliações
- The Associated Factors and Clinical Features Of.10Documento7 páginasThe Associated Factors and Clinical Features Of.10Vinay VivekAinda não há avaliações
- Chronic-Traumatic-Encephalopathy 2021 NeurochirurgieDocumento5 páginasChronic-Traumatic-Encephalopathy 2021 NeurochirurgieBruno MañonAinda não há avaliações
- Biomechanics of Musculoskeletal Pain Dynamics of The NeuromatrixDocumento12 páginasBiomechanics of Musculoskeletal Pain Dynamics of The NeuromatrixManuelAinda não há avaliações
- Peripheral - Nerve - Disorders - (PG - 24 25)Documento2 páginasPeripheral - Nerve - Disorders - (PG - 24 25)Fayeann Vedor LoriegaAinda não há avaliações
- Artigos Coderre1997Documento65 páginasArtigos Coderre1997JonasMarçaloAinda não há avaliações
- CCS Current Concepts 2k18Documento6 páginasCCS Current Concepts 2k18Guna KalanjiyamAinda não há avaliações
- AN C F P: EW Lassification For Acial AINDocumento4 páginasAN C F P: EW Lassification For Acial AINAkmal Niam FirdausiAinda não há avaliações
- Sci Managing Pain PDFDocumento16 páginasSci Managing Pain PDFPharmacist Ehab HammadAinda não há avaliações
- Neuropatia PerifericaDocumento11 páginasNeuropatia PerifericaJose Alejandro Bedoya SanchezAinda não há avaliações
- Lumbar Vertebral Stress Injuries in Fast BowlersDocumento8 páginasLumbar Vertebral Stress Injuries in Fast BowlersMd. Ariful IslamAinda não há avaliações
- Pelatihan Dry Needle 2022-CourseDocumento115 páginasPelatihan Dry Needle 2022-CoursebonangAinda não há avaliações
- Pain Classifitation 2 PDFDocumento11 páginasPain Classifitation 2 PDFAnnisa BrilianAinda não há avaliações
- Regeneration of Injured Skeletal Muscle After The Injury: Review ArticleDocumento9 páginasRegeneration of Injured Skeletal Muscle After The Injury: Review ArticleSahira Rivera DroguettAinda não há avaliações
- Commonwealth Ombudsman 1988Documento2 páginasCommonwealth Ombudsman 1988Terry LollbackAinda não há avaliações
- Molloy MartialArtsMateriality 2008Documento20 páginasMolloy MartialArtsMateriality 2008Terry LollbackAinda não há avaliações
- Recognition of Foreign DivorcesDocumento19 páginasRecognition of Foreign DivorcesTerry LollbackAinda não há avaliações
- Separation of Powers in The Australian ConstitutioDocumento19 páginasSeparation of Powers in The Australian ConstitutioTerry LollbackAinda não há avaliações
- POSSIBLE GUIDANCE FROM Roman LawDocumento14 páginasPOSSIBLE GUIDANCE FROM Roman LawTerry LollbackAinda não há avaliações
- MOLLOY SwordsSwordsmanshipAegean 2010Documento27 páginasMOLLOY SwordsSwordsmanshipAegean 2010Terry LollbackAinda não há avaliações
- New Community Radio Service For Oatlands1996Documento1 páginaNew Community Radio Service For Oatlands1996Terry LollbackAinda não há avaliações
- USQ Library - Harvard Referencing Guide November 2017Documento37 páginasUSQ Library - Harvard Referencing Guide November 2017ICEBOYAinda não há avaliações
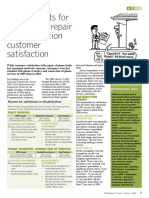
- 1996mixed Results For Phone Fault Repair and Connection Customer SatisfactionDocumento1 página1996mixed Results For Phone Fault Repair and Connection Customer SatisfactionTerry LollbackAinda não há avaliações
- 1996mixed Results For Phone Fault Repair and Connection Customer SatisfactionDocumento1 página1996mixed Results For Phone Fault Repair and Connection Customer SatisfactionTerry LollbackAinda não há avaliações
- USQ Library - Harvard Referencing Guide November 2017Documento37 páginasUSQ Library - Harvard Referencing Guide November 2017ICEBOYAinda não há avaliações
- Job DescriptionDocumento3 páginasJob DescriptionTerry LollbackAinda não há avaliações
- Creating Long Term Marketing RelationshipsDocumento24 páginasCreating Long Term Marketing RelationshipsTerry LollbackAinda não há avaliações
- Gen F QLD Stat DecDocumento1 páginaGen F QLD Stat DecTerry LollbackAinda não há avaliações
- StatisticsDocumento12 páginasStatisticsTerry LollbackAinda não há avaliações
- Filipinos in Nueva Espaã A: Filipino-Mexican Relations, Mestizaje, and Identity in Colonial and Contemporary MexicoDocumento29 páginasFilipinos in Nueva Espaã A: Filipino-Mexican Relations, Mestizaje, and Identity in Colonial and Contemporary MexicoTerry LollbackAinda não há avaliações
- Sample Cover Letter Financial PlannerDocumento2 páginasSample Cover Letter Financial PlannerTerry LollbackAinda não há avaliações
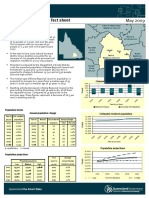
- Roma Regional Council PDFDocumento2 páginasRoma Regional Council PDFTerry LollbackAinda não há avaliações
- Housing Market Update: Property Investor SummitDocumento35 páginasHousing Market Update: Property Investor SummitTerry LollbackAinda não há avaliações
- Position Description Student Recruitment and Marketing Manager CHC OperationsDocumento6 páginasPosition Description Student Recruitment and Marketing Manager CHC OperationsTerry LollbackAinda não há avaliações
- Nla - News Article13325849.3 LollbackDocumento1 páginaNla - News Article13325849.3 LollbackTerry LollbackAinda não há avaliações
- Quick Reference Guide For Agents: Be What Want To BeDocumento16 páginasQuick Reference Guide For Agents: Be What Want To BeTerry LollbackAinda não há avaliações
- Cqu StudyDocumento1 páginaCqu StudyTerry LollbackAinda não há avaliações
- Bang Bang He Shot Me Down Can The Pistol Be Studied As A Historic European Martial ArtDocumento5 páginasBang Bang He Shot Me Down Can The Pistol Be Studied As A Historic European Martial ArtTerry LollbackAinda não há avaliações
- Crawford School - Deputy Manager International Exec Ed - Position Description PEWR (53066)Documento3 páginasCrawford School - Deputy Manager International Exec Ed - Position Description PEWR (53066)Terry LollbackAinda não há avaliações
- Depot - Wheelie Bin Request FormDocumento1 páginaDepot - Wheelie Bin Request FormTerry LollbackAinda não há avaliações
- Assignment Extention Form 2016Documento1 páginaAssignment Extention Form 2016Terry LollbackAinda não há avaliações
- Nijinda Durlga Hire FormDocumento11 páginasNijinda Durlga Hire FormTerry LollbackAinda não há avaliações
- Hepatic EncephalopatyDocumento15 páginasHepatic EncephalopatyJariza Daryl Tamang MejiaAinda não há avaliações
- Pre-Participation Screening: The Use of Fundamental Movements As An Assessment of Function - Part 2Documento8 páginasPre-Participation Screening: The Use of Fundamental Movements As An Assessment of Function - Part 2gogo36Ainda não há avaliações
- Dental Traumatology-Medicolegal Aspects (Indian Perspective)Documento6 páginasDental Traumatology-Medicolegal Aspects (Indian Perspective)akish4uAinda não há avaliações
- PariyaramDocumento30 páginasPariyaramModi EmAinda não há avaliações
- Calvert Cognitive Analytic TherapyDocumento25 páginasCalvert Cognitive Analytic TherapyldelblancodiezAinda não há avaliações
- Healthcareer InterviewquestionsandanswersDocumento7 páginasHealthcareer Interviewquestionsandanswersapi-256766284Ainda não há avaliações
- Plasma Terminal Half-Life: 2004 Blackwell Publishing LTD 427Documento13 páginasPlasma Terminal Half-Life: 2004 Blackwell Publishing LTD 427alibaba_1976Ainda não há avaliações
- VOYA USG Accident-Hospital IndemnityDocumento37 páginasVOYA USG Accident-Hospital IndemnityDavid BriggsAinda não há avaliações
- Roles and Responsibilities of The First AiderDocumento8 páginasRoles and Responsibilities of The First AiderPascual Ronald PatrickAinda não há avaliações
- Vitamin B 12 Fo Late DeficiencyDocumento14 páginasVitamin B 12 Fo Late DeficiencyAnghelo Aldair Velásquez CarrilloAinda não há avaliações
- Basic (Level IV) Trauma Facility CriteriaDocumento6 páginasBasic (Level IV) Trauma Facility CriteriaPiet Pogen PoelAinda não há avaliações
- Kala Azar EthiopiaDocumento11 páginasKala Azar EthiopiaPrabir Kumar ChatterjeeAinda não há avaliações
- Bedah - Buerger's DiseaseDocumento20 páginasBedah - Buerger's DiseaseDessy KusumadewiAinda não há avaliações
- Compartment SyndromeDocumento24 páginasCompartment SyndromeDexter BluesAinda não há avaliações
- Face Forward David and Deborah Alessi Disucuss Their Discuss Their Foundation's Upcoming Venetian MasquaradeDocumento2 páginasFace Forward David and Deborah Alessi Disucuss Their Discuss Their Foundation's Upcoming Venetian MasquaradeBeverlyHillsWeeklyAinda não há avaliações
- Antihistamines (Hayfever) and BreastfeedingDocumento2 páginasAntihistamines (Hayfever) and BreastfeedingEzraGoenadiAinda não há avaliações
- Blessed Dementia ScaleDocumento2 páginasBlessed Dementia ScaleAbdur RasyidAinda não há avaliações
- Hospital PharmacyDocumento13 páginasHospital PharmacySridivya SrihariAinda não há avaliações
- Transtracheal Wash and Bronchoalveolar Lavage: Maureen D. Finke, DVM, DACVIMDocumento4 páginasTranstracheal Wash and Bronchoalveolar Lavage: Maureen D. Finke, DVM, DACVIMSandra Putri DewiAinda não há avaliações