Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Grade 11 Topic TestsDocumento100 páginasGrade 11 Topic TestsKïm MugarapajiwaAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Biotechnology and Its ApplicationsDocumento2 páginasBiotechnology and Its ApplicationsEunice BasarioAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Cell and Molecular BiologyDocumento4 páginasCell and Molecular BiologyRea Joyce AldefollaAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- Clinical Manifestation of Oral TuberculosisDocumento6 páginasClinical Manifestation of Oral TuberculosisSasa AprilaAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Anti Diabetik A Oral: Dr. Theodorus, Mmedsc Staf Bagian Farmakologi FK UnsriDocumento30 páginasAnti Diabetik A Oral: Dr. Theodorus, Mmedsc Staf Bagian Farmakologi FK UnsriDewi Putri Lenggo GeniAinda não há avaliações
- Microbiology Sheet MCQ - Part 1Documento12 páginasMicrobiology Sheet MCQ - Part 1MahmOod Gh100% (3)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Chemotherapeutic Agents or Anti-MicrobialsDocumento36 páginasChemotherapeutic Agents or Anti-MicrobialsPROF DR SHAHMURADAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- SS2 Second Term Biology NoteDocumento41 páginasSS2 Second Term Biology NotereoxwillAinda não há avaliações
- Stages of Fetal Development FinalDocumento43 páginasStages of Fetal Development Finalsanthiyasandy100% (6)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- Ale Many 2014Documento37 páginasAle Many 2014Tatiane RibeiroAinda não há avaliações
- 6.4 LP Food DigestionDocumento6 páginas6.4 LP Food DigestionMiNH HayatAinda não há avaliações
- General Biology 1 Workbook Pages 43 52Documento12 páginasGeneral Biology 1 Workbook Pages 43 52R VHIAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
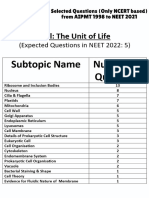
- Cell - The Unit of Life - NCERT Based PYQsDocumento9 páginasCell - The Unit of Life - NCERT Based PYQsAkhil singhAinda não há avaliações
- Peripheral Nerve Injuries: Michael D. Robinson, M.D. Phillip R. Bryant, D.ODocumento156 páginasPeripheral Nerve Injuries: Michael D. Robinson, M.D. Phillip R. Bryant, D.OejekimAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- ENDOSIGN Review v0 EdmvDocumento33 páginasENDOSIGN Review v0 EdmvMavi Camarasa SabaterAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- A Tool For The Analysis of Chromosomes: Karyotype: Taxon June 2016Documento8 páginasA Tool For The Analysis of Chromosomes: Karyotype: Taxon June 2016Kelly Rios ZapataAinda não há avaliações
- Sample Ch05Documento53 páginasSample Ch05mb_13_throwawayAinda não há avaliações
- Human Anatomy and PhysiologyDocumento136 páginasHuman Anatomy and PhysiologyLuis Margarejo91% (11)
- 2ND Gen Bio Prelim NotesDocumento8 páginas2ND Gen Bio Prelim NotesRalph RadazaAinda não há avaliações
- Heredity and Variation.Documento6 páginasHeredity and Variation.AnweAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Module 9 - Earth & Life ScienceDocumento25 páginasModule 9 - Earth & Life ScienceRosalyn Marie Sugay64% (14)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- BiografieDocumento73 páginasBiografieAna-Maria PantazicaAinda não há avaliações
- Biology 2EE3 - Intro To Micro & Biotech (1-3)Documento9 páginasBiology 2EE3 - Intro To Micro & Biotech (1-3)VeryMerryAinda não há avaliações
- Animal Kingdom Classification GuideDocumento91 páginasAnimal Kingdom Classification GuideJoanna Susan JojiAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- SR5 TOOL Chrome Flesh IndexDocumento2 páginasSR5 TOOL Chrome Flesh IndexBeki LokaAinda não há avaliações
- Entrance Test For M.Phil/Ph.D. (Biotechnology) (Sample Paper)Documento19 páginasEntrance Test For M.Phil/Ph.D. (Biotechnology) (Sample Paper)Rehaan FayazAinda não há avaliações
- BIO311D SPR 22 WK4 Discussion - AssignmentDocumento5 páginasBIO311D SPR 22 WK4 Discussion - AssignmentAvin deSilvaAinda não há avaliações
- Qku3093 Sports Nutrition NotesDocumento19 páginasQku3093 Sports Nutrition NotesAizat Farhan100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- ManualGoodFeb17 2004 TextOnlyDocumento132 páginasManualGoodFeb17 2004 TextOnlyIvonne JalcaAinda não há avaliações
- Jurnal: Identifikasi Kromosom Homolog Melalui Deteksi Pada Tanaman Bawang MerahDocumento9 páginasJurnal: Identifikasi Kromosom Homolog Melalui Deteksi Pada Tanaman Bawang MerahImaniar FitriatasyaVWAinda não há avaliações