Você também pode gostar
- FormOP 03 OSS NHB ANCLRY Rev8 6172022Documento2 páginasFormOP 03 OSS NHB ANCLRY Rev8 6172022dumalneghrh 2017Ainda não há avaliações
- Report 57Documento2 páginasReport 57Dy KashikaAinda não há avaliações
- Republic of The Philippines Department of Health Health Facilities and Services Regulatory BureauDocumento3 páginasRepublic of The Philippines Department of Health Health Facilities and Services Regulatory Bureaumartin marasigan mem hospitalAinda não há avaliações
- Jacob Final Bill Receipt - September - 2023Documento1 páginaJacob Final Bill Receipt - September - 20234pillar AssistAinda não há avaliações
- Yuana Saraswati MerthaDocumento4 páginasYuana Saraswati MerthaLosta NataAinda não há avaliações
- Region Compare SFY 10-11Documento5 páginasRegion Compare SFY 10-11rkarlinAinda não há avaliações
- COTATION AFCOTT CAM SARL - Fr.enDocumento1 páginaCOTATION AFCOTT CAM SARL - Fr.enMichel erickson talom waboAinda não há avaliações
- E Liwag 01312007 OLDDocumento2 páginasE Liwag 01312007 OLDdaqs06Ainda não há avaliações
- Approval Memo...Documento4 páginasApproval Memo...Salifu AbdulAinda não há avaliações
- BudgetDocumento7 páginasBudgetvasanthgurusamynsAinda não há avaliações
- Admissions 2020 - General Category FeesDocumento19 páginasAdmissions 2020 - General Category FeesalishAinda não há avaliações
- In The Name of Allah, The Gracious, The MercifulDocumento17 páginasIn The Name of Allah, The Gracious, The MercifulZia Ul Haq BandeshaAinda não há avaliações
- Stategic Accounting For Decision Making: Answer 1Documento12 páginasStategic Accounting For Decision Making: Answer 1abhigoldyAinda não há avaliações
- 14 - Accounting 4 DepreciationDocumento22 páginas14 - Accounting 4 DepreciationKAMAL POKHRELAinda não há avaliações
- Star Health InsuranceDocumento2 páginasStar Health InsurancevinujohnpanickerAinda não há avaliações
- Income and Expenditure Report: Business Unit: PKA Country: Marie Stopes Society Pakistan Cost Center JhangDocumento34 páginasIncome and Expenditure Report: Business Unit: PKA Country: Marie Stopes Society Pakistan Cost Center JhangMuhammad Hasnain SikanderAinda não há avaliações
- ACADEMIC YEAR - 2015-2016: Subject Code: Bhm206 EXAM DATE: 23.11.2015Documento4 páginasACADEMIC YEAR - 2015-2016: Subject Code: Bhm206 EXAM DATE: 23.11.2015raulAinda não há avaliações
- The University of Lahore Lahore Business School Fee Structure Fall 2019 BBADocumento5 páginasThe University of Lahore Lahore Business School Fee Structure Fall 2019 BBAilyas muhammadAinda não há avaliações
- Abdullah MahmoodDocumento6 páginasAbdullah Mahmoodparimala8777Ainda não há avaliações
- Health MaxDocumento1 páginaHealth MaxHashan SandeepaAinda não há avaliações
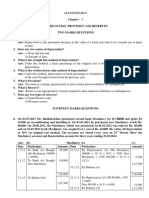
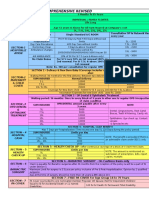
- II PU AccountsDocumento30 páginasII PU AccountsJanani Priya100% (2)
- Mahendra Kumar Copy of Investment Declaration Fy 17-18Documento2 páginasMahendra Kumar Copy of Investment Declaration Fy 17-18mahendraAinda não há avaliações
- Invoice: Cv. Sederhana Baru MedikaDocumento33 páginasInvoice: Cv. Sederhana Baru MedikayuniaovtsrAinda não há avaliações
- Procurement For Isolation Area For 13 PatientsDocumento21 páginasProcurement For Isolation Area For 13 PatientsSample BakeshopAinda não há avaliações
- Course Fees: Manipal CampusDocumento17 páginasCourse Fees: Manipal CampusrajatAinda não há avaliações
- Financial Counseling For IVF (Resident)Documento2 páginasFinancial Counseling For IVF (Resident)SantosoAinda não há avaliações
- FM09-CH 11Documento5 páginasFM09-CH 11Mukul KadyanAinda não há avaliações
- ch20 (改)Documento21 páginasch20 (改)林義哲Ainda não há avaliações
- ACADEMIC YEAR - 2013-2014: Subject Code: Bhm206 EXAM DATE: 25.11.2013Documento4 páginasACADEMIC YEAR - 2013-2014: Subject Code: Bhm206 EXAM DATE: 25.11.2013raulAinda não há avaliações
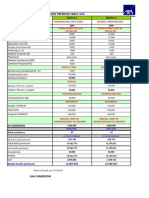
- Comp One Pager With Premium ChartDocumento3 páginasComp One Pager With Premium ChartnithinAinda não há avaliações
- 2009 Hosp BudgetDocumento5 páginas2009 Hosp BudgetfaseeAinda não há avaliações
- dDOH AO 28s. 2008Documento6 páginasdDOH AO 28s. 2008Rachelle SigueAinda não há avaliações
- Perkiraan Biaya Operasi Rs - Usada Insani: Total Biaya Diluar Alat 17,660,000Documento8 páginasPerkiraan Biaya Operasi Rs - Usada Insani: Total Biaya Diluar Alat 17,660,000Vincent ArlouwAinda não há avaliações
- Detailed Financial Physical Performance TargetsDocumento1 páginaDetailed Financial Physical Performance TargetsReslyn Yanoc100% (1)
- Rka Bok 2018 Final Update 1 - 2Documento233 páginasRka Bok 2018 Final Update 1 - 2asmiyatunAinda não há avaliações
- Medical Book QuotDocumento1 páginaMedical Book QuotJaved Noor Muhammad GabaAinda não há avaliações
- Accountancy Set 3 Ms - DocxDocumento7 páginasAccountancy Set 3 Ms - DocxKunal GauravAinda não há avaliações
- NP Ex365 2021 Cs1-4a Sophiakindiak 2Documento8 páginasNP Ex365 2021 Cs1-4a Sophiakindiak 2api-682588816Ainda não há avaliações
- Unlimited 5lkDocumento2 páginasUnlimited 5lkHashan SandeepaAinda não há avaliações
- Application Fee Details For (Manufacturing, Retail and Wholesale Licence)Documento4 páginasApplication Fee Details For (Manufacturing, Retail and Wholesale Licence)mass giridihAinda não há avaliações
- Managerial AnalysisDocumento5 páginasManagerial AnalysisIsaac OmwengaAinda não há avaliações
- DepreciationDocumento3 páginasDepreciationSumanth KumarAinda não há avaliações
- Annexure 1Documento1 páginaAnnexure 1pauomihaldarAinda não há avaliações
- Anita Dewi Lestari - MCU - Eka 1Documento4 páginasAnita Dewi Lestari - MCU - Eka 1Chandra SaputraAinda não há avaliações
- Bm. Gupta Hospital Pvt. LTD: 9 X-Ray Chest P/A View (1 - 250)Documento1 páginaBm. Gupta Hospital Pvt. LTD: 9 X-Ray Chest P/A View (1 - 250)Abhijit PandeyAinda não há avaliações
- Ilovepdf MergedDocumento3 páginasIlovepdf MergedPrabin T PrasadAinda não há avaliações
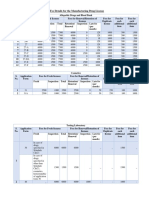
- (Sample Format) For Livestock Raising Only - Hog Raising: Farm Plan and BudgetDocumento7 páginas(Sample Format) For Livestock Raising Only - Hog Raising: Farm Plan and BudgetAlo RioAinda não há avaliações
- LSB Budget 2020Documento7 páginasLSB Budget 2020Divine Grace SamortinAinda não há avaliações
- Invoice-InV NCI Pro546Documento2 páginasInvoice-InV NCI Pro546Nci Centre KalimantanAinda não há avaliações
- Cup Pa ManiaDocumento2 páginasCup Pa ManiadeepaksikriAinda não há avaliações
- Benchmarking: - Process - People - Sample OutputDocumento12 páginasBenchmarking: - Process - People - Sample Outputotis lynchAinda não há avaliações
- Estimasi Service & Perbaikan: (Total Sparepart Dan Jasa)Documento1 páginaEstimasi Service & Perbaikan: (Total Sparepart Dan Jasa)Hari AbriantoAinda não há avaliações
- Project Telehealth - Health at Home: Equipment InformationDocumento1 páginaProject Telehealth - Health at Home: Equipment InformationSenapati Prabhupada DasAinda não há avaliações
- Amendment Operational Guidelines NLMDocumento4 páginasAmendment Operational Guidelines NLMThe Match PointAinda não há avaliações
- Updated SME Luxe Proposal For Triforce GlobalDocumento21 páginasUpdated SME Luxe Proposal For Triforce GlobalallangreslyAinda não há avaliações
- San Pedro Hospital of Davao: Statement of Account SOA Reference No.: 2018-221260Documento1 páginaSan Pedro Hospital of Davao: Statement of Account SOA Reference No.: 2018-221260Patricia Nicole Balgoa100% (3)
- Notes To Account Pendapatan: Jagung Manis - AssumptionsDocumento4 páginasNotes To Account Pendapatan: Jagung Manis - AssumptionsNik AzizAinda não há avaliações
- HPA 14 Assignemnt Due November 16thDocumento5 páginasHPA 14 Assignemnt Due November 16thcAinda não há avaliações
- Case Studies in Not-for-Profit Accounting and AuditingNo EverandCase Studies in Not-for-Profit Accounting and AuditingAinda não há avaliações
- Individual Performance Commitment and Review (Ipcr)Documento2 páginasIndividual Performance Commitment and Review (Ipcr)Reuben Jr UmallaAinda não há avaliações
- As of - : 2019 School Based Immunization Program ReportDocumento28 páginasAs of - : 2019 School Based Immunization Program ReportReuben Jr UmallaAinda não há avaliações
- Morb, F1+, MortNat, A1Prog, Demo, M2, A1 Program FormsDocumento30 páginasMorb, F1+, MortNat, A1Prog, Demo, M2, A1 Program FormsReuben Jr UmallaAinda não há avaliações
- Quarantine Facility Assessment Tool 2Documento2 páginasQuarantine Facility Assessment Tool 2Reuben Jr UmallaAinda não há avaliações
- Mapping and Analysis of Indigenous Gover PDFDocumento205 páginasMapping and Analysis of Indigenous Gover PDFReuben Jr UmallaAinda não há avaliações
- FNH 12 PDFDocumento6 páginasFNH 12 PDFReuben Jr UmallaAinda não há avaliações
- Community Health Workers PDFDocumento42 páginasCommunity Health Workers PDFReuben Jr UmallaAinda não há avaliações
- Nutrition Month Celebration Activities 2019finaleDocumento4 páginasNutrition Month Celebration Activities 2019finaleReuben Jr UmallaAinda não há avaliações
- Research Proposal MatrixDocumento2 páginasResearch Proposal MatrixReuben Jr UmallaAinda não há avaliações
- Globe BillDocumento2 páginasGlobe BillReuben Jr Umalla0% (1)
- BSU-OU Course ChecklistDocumento9 páginasBSU-OU Course ChecklistReuben Jr UmallaAinda não há avaliações
- Census Template-Rev 1 Reg 1Documento2 páginasCensus Template-Rev 1 Reg 1Reuben Jr UmallaAinda não há avaliações
- Integral Youth Ministry Meeting APRIL 3, 2016: PresentDocumento1 páginaIntegral Youth Ministry Meeting APRIL 3, 2016: PresentReuben Jr UmallaAinda não há avaliações
- LGU PSND 2017 Convention InvitationDocumento6 páginasLGU PSND 2017 Convention InvitationReuben Jr UmallaAinda não há avaliações
- Midwife FormDocumento7 páginasMidwife FormReuben Jr UmallaAinda não há avaliações
- Tubigon Bohol S Nutrition Programs and Best PracticesDocumento27 páginasTubigon Bohol S Nutrition Programs and Best PracticesReuben Jr UmallaAinda não há avaliações
- Follow-Up Provincial Doh Office: Provincial Epidemiology and Surveillance UnitDocumento2 páginasFollow-Up Provincial Doh Office: Provincial Epidemiology and Surveillance UnitReuben Jr UmallaAinda não há avaliações
- Scholastica: Mock 1Documento14 páginasScholastica: Mock 1Fatema KhatunAinda não há avaliações
- Rifle May 2015 USADocumento72 páginasRifle May 2015 USAhanshcAinda não há avaliações
- Bom Details FormatDocumento6 páginasBom Details FormatPrince MittalAinda não há avaliações
- Model 255 Aerosol Generator (Metone)Documento20 páginasModel 255 Aerosol Generator (Metone)Ali RizviAinda não há avaliações
- BSC HTM - TourismDocumento4 páginasBSC HTM - Tourismjaydaman08Ainda não há avaliações
- Sveba Dahlen - SRP240Documento16 páginasSveba Dahlen - SRP240Paola MendozaAinda não há avaliações
- Z-Purlins: Technical DocumentationDocumento11 páginasZ-Purlins: Technical Documentationardit bedhiaAinda não há avaliações
- Dermatology Skin in Systemic DiseaseDocumento47 páginasDermatology Skin in Systemic DiseaseNariska CooperAinda não há avaliações
- Lecture2 GranulopoiesisDocumento9 páginasLecture2 GranulopoiesisAfifa Prima GittaAinda não há avaliações
- Unsuccessful MT-SM DeliveryDocumento2 páginasUnsuccessful MT-SM DeliveryPitam MaitiAinda não há avaliações
- C2 - Conveyors Diagram: Peso de Faja Longitud de CargaDocumento1 páginaC2 - Conveyors Diagram: Peso de Faja Longitud de CargaIvan CruzAinda não há avaliações
- Biography Thesis ExamplesDocumento7 páginasBiography Thesis Examplesreneewardowskisterlingheights100% (2)
- Design of Penstock: Reference Code:IS 11639 (Part 2)Documento4 páginasDesign of Penstock: Reference Code:IS 11639 (Part 2)sunchitk100% (3)
- Continue Practice Exam Test Questions Part 1 of The SeriesDocumento7 páginasContinue Practice Exam Test Questions Part 1 of The SeriesKenn Earl Bringino VillanuevaAinda não há avaliações
- Where We Are in Place and Time "We Are Part of The Universe and Feel Compelled To Explore It."Documento1 páginaWhere We Are in Place and Time "We Are Part of The Universe and Feel Compelled To Explore It."Safia-umm Suhaim- FareedAinda não há avaliações
- Physics Blue Print 1 Class XI Half Yearly 23Documento1 páginaPhysics Blue Print 1 Class XI Half Yearly 23Nilima Aparajita SahuAinda não há avaliações
- QSP 04bDocumento35 páginasQSP 04bakrastogi94843Ainda não há avaliações
- Modlist - Modlist 1.4Documento145 páginasModlist - Modlist 1.4Tattorin vemariaAinda não há avaliações
- Siemens Make Motor Manual PDFDocumento10 páginasSiemens Make Motor Manual PDFArindam SamantaAinda não há avaliações
- Clark SM 616 Service ManualDocumento20 páginasClark SM 616 Service Manualenid100% (55)
- Student Exploration: Inclined Plane - Simple MachineDocumento9 páginasStudent Exploration: Inclined Plane - Simple MachineLuka MkrtichyanAinda não há avaliações
- Catify To Satisfy - Simple Solutions For Creating A Cat-Friendly Home (PDFDrive)Documento315 páginasCatify To Satisfy - Simple Solutions For Creating A Cat-Friendly Home (PDFDrive)Paz Libros100% (2)
- Escaner Electromagnético de Faja Transportadora-Steel SPECTDocumento85 páginasEscaner Electromagnético de Faja Transportadora-Steel SPECTEdwin Alfredo Eche QuirozAinda não há avaliações
- IEC TC 56 Dependability PDFDocumento8 páginasIEC TC 56 Dependability PDFsaospieAinda não há avaliações
- Cummin C1100 Fuel System Flow DiagramDocumento8 páginasCummin C1100 Fuel System Flow DiagramDaniel KrismantoroAinda não há avaliações
- Miniature Daisy: Crochet Pattern & InstructionsDocumento8 páginasMiniature Daisy: Crochet Pattern & Instructionscaitlyn g100% (1)
- Tool Charts PDFDocumento3 páginasTool Charts PDFtebengz100% (2)
- 2011-2012 - Medical - DirectoryDocumento112 páginas2011-2012 - Medical - DirectoryЈелена КошевићAinda não há avaliações
- Workbook Group TheoryDocumento62 páginasWorkbook Group TheoryLi NguyenAinda não há avaliações
- World Insurance Report 2017Documento36 páginasWorld Insurance Report 2017deolah06Ainda não há avaliações