Você também pode gostar
- Ni Kadek 1Documento1 páginaNi Kadek 1Nikadek Ayu Dwi LestariAinda não há avaliações
- Revista Brasileira DE AnestesiologiaDocumento12 páginasRevista Brasileira DE AnestesiologiaNikadek Ayu Dwi LestariAinda não há avaliações
- Artikel Proposal 1Documento10 páginasArtikel Proposal 1Nikadek Ayu Dwi LestariAinda não há avaliações
- Jurnal KadekDocumento6 páginasJurnal KadekNikadek Ayu Dwi LestariAinda não há avaliações
- SIRS Is Valid in Discriminating Between Severe and Moderate Diabetic Foot InfectionsDocumento6 páginasSIRS Is Valid in Discriminating Between Severe and Moderate Diabetic Foot InfectionsNikadek Ayu Dwi LestariAinda não há avaliações
- Tugas Bahasa Inggris KadekDocumento2 páginasTugas Bahasa Inggris KadekNikadek Ayu Dwi LestariAinda não há avaliações
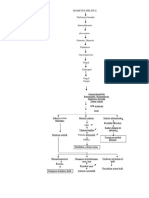
- Pathway ArfDocumento1 páginaPathway ArfNikadek Ayu Dwi LestariAinda não há avaliações
- Internet Psycho-Education Programs Improve Outcomes in Youth With Type 1 DiabetesDocumento8 páginasInternet Psycho-Education Programs Improve Outcomes in Youth With Type 1 DiabetesNikadek Ayu Dwi LestariAinda não há avaliações
- Artikel KadekDocumento17 páginasArtikel KadekNikadek Ayu Dwi LestariAinda não há avaliações
- Tugas Bahasa Inggris KadekDocumento2 páginasTugas Bahasa Inggris KadekNikadek Ayu Dwi LestariAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Histopath-Prelim ReviewerDocumento10 páginasHistopath-Prelim ReviewerKhey AgamAinda não há avaliações
- Table of Surgical)Documento98 páginasTable of Surgical)Bilal AhmadAinda não há avaliações
- Best Practice Diagnostic Guidelines For Patients Presenting With Breast Symptoms PDFDocumento60 páginasBest Practice Diagnostic Guidelines For Patients Presenting With Breast Symptoms PDFfauziafahmi95Ainda não há avaliações
- Soft Tissue Biopsy Needles - BR - ENDocumento20 páginasSoft Tissue Biopsy Needles - BR - ENAgung WibowoAinda não há avaliações
- CPT Coding Practice AnswersDocumento17 páginasCPT Coding Practice AnswersTannu SamadAinda não há avaliações
- Velscope Oral PremalignancyDocumento5 páginasVelscope Oral PremalignancySusanaSanoAinda não há avaliações
- 6.musculoskeletal TumorsDocumento110 páginas6.musculoskeletal Tumorslina jamalAinda não há avaliações
- BSU-CON Case Study on Breast Cancer Stage IIIBDocumento106 páginasBSU-CON Case Study on Breast Cancer Stage IIIBfLOR_ZIANE_MAEAinda não há avaliações
- Clinical Presentation, Histopathology, Diagnostic Evaluation, and Staging of Soft Tissue Sarcoma - UpToDateDocumento36 páginasClinical Presentation, Histopathology, Diagnostic Evaluation, and Staging of Soft Tissue Sarcoma - UpToDateKevin AdrianAinda não há avaliações
- (Atlas of Anatomic Pathology) Scott R. Owens, Henry D. Appelman (Auth.) - Atlas of Esophagus and Stomach Pathology-Springer-Verlag New York (2014)Documento191 páginas(Atlas of Anatomic Pathology) Scott R. Owens, Henry D. Appelman (Auth.) - Atlas of Esophagus and Stomach Pathology-Springer-Verlag New York (2014)Amanda Teaca100% (1)
- Gastric Carcinoma: Professor Ravi KantDocumento44 páginasGastric Carcinoma: Professor Ravi KantVasanth MalagiAinda não há avaliações
- Chapter 1-Basic Word Structure - Language of MedicineDocumento12 páginasChapter 1-Basic Word Structure - Language of Medicineapi-1982440667% (6)
- DOJ Complaint Alleges Medical Malpractice Resulting in DeathDocumento4 páginasDOJ Complaint Alleges Medical Malpractice Resulting in DeathSulong Pinas JRAinda não há avaliações
- Breast Lump Prognosis Prediction/TITLEDocumento30 páginasBreast Lump Prognosis Prediction/TITLETony DawaAinda não há avaliações
- Investigatory Project On CANCERDocumento15 páginasInvestigatory Project On CANCERSreeja SwainAinda não há avaliações
- Overview of Breast Cancer.3Documento5 páginasOverview of Breast Cancer.3Kurnia AlkatiriAinda não há avaliações
- Q4 G7 Reviewer For HealthDocumento9 páginasQ4 G7 Reviewer For HealthAine YahAinda não há avaliações
- Uterine Sarcoma Cancer - Com For PatientsDocumento40 páginasUterine Sarcoma Cancer - Com For PatientsSarah MuharomahAinda não há avaliações
- Lung Cancer (Nursing Care)Documento5 páginasLung Cancer (Nursing Care)heiyuAinda não há avaliações
- Blood Tube Collection GuideDocumento365 páginasBlood Tube Collection GuideFeliciadlTAinda não há avaliações
- Children and Young People With Cancer:: A Parent's GuideDocumento37 páginasChildren and Young People With Cancer:: A Parent's GuideCatarina CostaAinda não há avaliações
- Leiomyosarcoma of The BoneDocumento5 páginasLeiomyosarcoma of The BonedrjorgewtorresAinda não há avaliações
- ASSISTING IN BONE MARROW ASPIRATION (2) .Doc Revised. ADocumento9 páginasASSISTING IN BONE MARROW ASPIRATION (2) .Doc Revised. ARiza Angela BarazanAinda não há avaliações
- Gastritis - Etiology and Diagnosis - UpToDateDocumento10 páginasGastritis - Etiology and Diagnosis - UpToDateLizbeth Navarrete SierraAinda não há avaliações
- Krithika Shankar Updated Resume 2023Documento8 páginasKrithika Shankar Updated Resume 2023Katrina ReyesAinda não há avaliações
- Ingles 2Documento4 páginasIngles 2Natalia AriasAinda não há avaliações
- Bone Marrow AspirationDocumento43 páginasBone Marrow AspirationDr. Pawan KumarAinda não há avaliações
- LAB-Histopath Midterms 01Documento5 páginasLAB-Histopath Midterms 01Jashmine May TadinaAinda não há avaliações
- W Biod05Documento13 páginasW Biod05Эма СэмAinda não há avaliações
- Colitis PDFDocumento11 páginasColitis PDFicoanamareAinda não há avaliações