Você também pode gostar
- ENG An.6 GI-imagingDocumento45 páginasENG An.6 GI-imagingSimina ÎntunericAinda não há avaliações
- Abdominal SignDocumento85 páginasAbdominal Signnovitafitri123Ainda não há avaliações
- Image Interpretation 4 (Autosaved) SssDocumento169 páginasImage Interpretation 4 (Autosaved) SssifeanyiAinda não há avaliações
- Radiographic Anatomy of Gastrointestinal Tract: Dr. Kikomeko Sharif Department of Radiology Iuiu-Habib Medical SchoolDocumento55 páginasRadiographic Anatomy of Gastrointestinal Tract: Dr. Kikomeko Sharif Department of Radiology Iuiu-Habib Medical SchoolUsaid SulaimanAinda não há avaliações
- Radiology Examination For Tractus Digestivus Chairunnisa, Dr. SP - RadDocumento100 páginasRadiology Examination For Tractus Digestivus Chairunnisa, Dr. SP - RadDiana OCtavinaAinda não há avaliações
- Gastrointestinal Imaging AnatomyDocumento69 páginasGastrointestinal Imaging AnatomySari Prasili SuddinAinda não há avaliações
- X Ray DiscussionDocumento38 páginasX Ray DiscussionJINI JOSEPHAinda não há avaliações
- Radiology Gi 2017Documento108 páginasRadiology Gi 2017Ario LukasAinda não há avaliações
- Abdominal X-Rays: DR Fizzah ArifDocumento60 páginasAbdominal X-Rays: DR Fizzah ArifMurk NiazAinda não há avaliações
- Obstruction. DidacticsDocumento87 páginasObstruction. DidacticsJoher MendezAinda não há avaliações
- How To Read Chest Abdomen CT Scan X-RayDocumento86 páginasHow To Read Chest Abdomen CT Scan X-RaymuhammadfyAinda não há avaliações
- Abdomen XrayDocumento82 páginasAbdomen Xraypriyasureddi8004100% (2)
- 14 - Barium Studies For GIT With NotesDocumento50 páginas14 - Barium Studies For GIT With NotesSunil ThomasAinda não há avaliações
- Dr. Bryan - Abdomen PlainDocumento117 páginasDr. Bryan - Abdomen PlainnaynaAinda não há avaliações
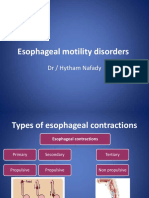
- Esophageal Motility Disorders: DR / Hytham NafadyDocumento31 páginasEsophageal Motility Disorders: DR / Hytham NafadyRabie MeramAinda não há avaliações
- Coass OmdDocumento47 páginasCoass OmdKevin SurjadiAinda não há avaliações
- Acute AbdomenDocumento117 páginasAcute Abdomenayundaafdal100% (1)
- AbdomenT PDFDocumento130 páginasAbdomenT PDFmuniraAinda não há avaliações
- TBL 3: Dysphagia: By: Anis, Aishah, Nubla, Hanafi, HidayahDocumento84 páginasTBL 3: Dysphagia: By: Anis, Aishah, Nubla, Hanafi, HidayahNadia RahimAinda não há avaliações
- Bachtiar Murtala: Department of Radiology Medical Faculty Hasanuddin UniversityDocumento102 páginasBachtiar Murtala: Department of Radiology Medical Faculty Hasanuddin UniversitynafisahAinda não há avaliações
- Barium StudyDocumento34 páginasBarium StudyJahanavi JaluAinda não há avaliações
- Abdomen Pelvis Acd Club-WPS OfficeDocumento31 páginasAbdomen Pelvis Acd Club-WPS OfficeTahaani Bilqis ZoraayaAinda não há avaliações
- Foto Polos Abdomen - PPTX William Bunga DatuDocumento39 páginasFoto Polos Abdomen - PPTX William Bunga DatuWilliam Bunga DatuAinda não há avaliações
- ENT RadiologiDocumento70 páginasENT RadiologiyowwwAinda não há avaliações
- Barium Swallow & Barium Meal Shubhashish MondalDocumento52 páginasBarium Swallow & Barium Meal Shubhashish MondalShubhashis MondalAinda não há avaliações
- BariumswallowDocumento48 páginasBariumswallowCintyaRolitaAinda não há avaliações
- Abdomen BOF 3Documento78 páginasAbdomen BOF 3BakingpancakesAinda não há avaliações
- Git Anomalies: DR Varun Bansal Dept of Radio-DiagnosisDocumento54 páginasGit Anomalies: DR Varun Bansal Dept of Radio-DiagnosisJoyce MedAinda não há avaliações
- ENT Radiology ADocumento64 páginasENT Radiology AMitulsinh M RavaljiAinda não há avaliações
- PEMERIKSAAN RADIOLOGI PADA GASTRITIS DAN ULKUS-edited2017Documento51 páginasPEMERIKSAAN RADIOLOGI PADA GASTRITIS DAN ULKUS-edited2017shrt gtAinda não há avaliações
- Kuliah KBK Tract GI Tract 2020Documento94 páginasKuliah KBK Tract GI Tract 2020Tasya SunandarAinda não há avaliações
- Ldcu Group 4 Buscaino April ShineDocumento57 páginasLdcu Group 4 Buscaino April ShineApril Shine BuscainoAinda não há avaliações
- Abdominal SIGN OF PEDIATRIC ABNORMALITIESDocumento35 páginasAbdominal SIGN OF PEDIATRIC ABNORMALITIESnovitafitri123Ainda não há avaliações
- Abnormal Bowel Gas PatternDocumento136 páginasAbnormal Bowel Gas PatternEdward ElricAinda não há avaliações
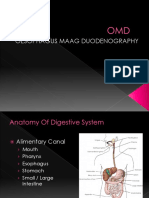
- Oesophagus Maag DuodenographyDocumento49 páginasOesophagus Maag DuodenographyEvan DionesiaAinda não há avaliações
- Ileus Pada Pediatrik: Syifa Sari Siregar 170100090Documento39 páginasIleus Pada Pediatrik: Syifa Sari Siregar 170100090AmardiasAinda não há avaliações
- From Doc Bandong's Own Words:: Shar 1 of 20Documento20 páginasFrom Doc Bandong's Own Words:: Shar 1 of 20sarguss14100% (1)
- Jurnal Radiologi NadiaDocumento46 páginasJurnal Radiologi NadiaNadia Rezky ElizaAinda não há avaliações
- Anatomi Radiologi Foto Polos AbdomenDocumento64 páginasAnatomi Radiologi Foto Polos AbdomenDesy Nurul AzizahAinda não há avaliações
- Git Investigations NEWDocumento50 páginasGit Investigations NEWbenak shivalingappaAinda não há avaliações
- Radiology Abdomen InterpretationsDocumento108 páginasRadiology Abdomen InterpretationsStudent100% (1)
- Fluoroscopic Investigations of The Gastrointestinal Tract: Pharynx, Oesophagus and StomachDocumento36 páginasFluoroscopic Investigations of The Gastrointestinal Tract: Pharynx, Oesophagus and StomachSatish PaswanAinda não há avaliações
- How To Read XRay AbdomenDocumento65 páginasHow To Read XRay AbdomenKlinik KDU100% (1)
- Radioanatomi Sistem PencernaanDocumento104 páginasRadioanatomi Sistem PencernaanRai adityaAinda não há avaliações
- Contrasted Studies GITDocumento91 páginasContrasted Studies GITolumAinda não há avaliações
- Case Report: Achalasia-Like Dysmotility Secondary To Oesophageal Involvement of SarcoidosisDocumento4 páginasCase Report: Achalasia-Like Dysmotility Secondary To Oesophageal Involvement of SarcoidosisDetry Kala'lembangAinda não há avaliações
- ABDOMINAL RadiographyDocumento147 páginasABDOMINAL RadiographyNematoda GgAinda não há avaliações
- 1 OMD, Indikasi, Dan Mekanisme Rujukan PanoramicDocumento57 páginas1 OMD, Indikasi, Dan Mekanisme Rujukan Panoramicgreg_enricoAinda não há avaliações
- Esophagus Symptoms and InvestigationDocumento7 páginasEsophagus Symptoms and InvestigationJinAinda não há avaliações
- Dasar Dasar Radiologi Digestive Dan Nefrourinari1Documento102 páginasDasar Dasar Radiologi Digestive Dan Nefrourinari1Mada Dwi Hari100% (1)
- Plain Film AbdomenDocumento90 páginasPlain Film AbdomenRapid Medicine100% (1)
- Imaging of Git & Hepatobiliary Systems CSLDocumento70 páginasImaging of Git & Hepatobiliary Systems CSLSara ManzoorAinda não há avaliações
- Intestinal ObstructionDocumento59 páginasIntestinal ObstructionBeyene FelekeAinda não há avaliações
- Entradiologya2 140402111623 Phpapp01Documento55 páginasEntradiologya2 140402111623 Phpapp01ibrahimAinda não há avaliações
- Raniê Ralph RadiologiaDocumento3 páginasRaniê Ralph RadiologiaAndré Luiz QueirozAinda não há avaliações
- Benign Disease of The Esophagus PDFDocumento4 páginasBenign Disease of The Esophagus PDFSpecialNameAinda não há avaliações
- AbdomenDocumento2 páginasAbdomenElizer Mario Pre RaboyAinda não há avaliações
- Gastrointestinal Imaging: Dr. Christina AndicaDocumento93 páginasGastrointestinal Imaging: Dr. Christina AndicaMirza SullivanAinda não há avaliações
- Nursing Assessment of The Gastrointestinal System: DR/ Nermen Abd ElftahDocumento94 páginasNursing Assessment of The Gastrointestinal System: DR/ Nermen Abd Elftah3amabelle arevalo100% (1)
- Pulmonary Pathology: Maria Sarah L. Lenon, MD, DPSPDocumento32 páginasPulmonary Pathology: Maria Sarah L. Lenon, MD, DPSPKATREEYA ELEONOR LIMSIAinda não há avaliações
- Olfaction PDFDocumento5 páginasOlfaction PDFjorgegrodl100% (1)
- Hemodynamics For The Bedside Nurse 1CEUDocumento7 páginasHemodynamics For The Bedside Nurse 1CEURN333100% (1)
- Jang 2015Documento9 páginasJang 2015Luis Alberto Carpio MorenoAinda não há avaliações
- Epker 1977Documento4 páginasEpker 1977leslie kalathilAinda não há avaliações
- Kapandji TrunkDocumento245 páginasKapandji TrunkVTZIOTZIAS90% (10)
- Estimation of Age of A Person From Examination of TeethDocumento48 páginasEstimation of Age of A Person From Examination of TeethhiranyaupadhyayaAinda não há avaliações
- 1000 MCQS - PAEDODONTICS, COMMUNITIY & PUBLIC HEALTH Plus September 2014 MCQsDocumento22 páginas1000 MCQS - PAEDODONTICS, COMMUNITIY & PUBLIC HEALTH Plus September 2014 MCQsHarjotBrar100% (2)
- Antihuman Globulin (Ahg) TestDocumento38 páginasAntihuman Globulin (Ahg) TestJerome ValerianoAinda não há avaliações
- Science Grade 3 LAS FnalDocumento13 páginasScience Grade 3 LAS FnalSan Isidro ISAinda não há avaliações
- The Hazards: OF Blood TransfusionDocumento7 páginasThe Hazards: OF Blood TransfusionPranjal Kr SahariaAinda não há avaliações
- PolycythemiaDocumento2 páginasPolycythemiaDina AssefaAinda não há avaliações
- Physiology of Hemodynamics-1: Dr. Ghaleb AlmekhlafiDocumento52 páginasPhysiology of Hemodynamics-1: Dr. Ghaleb AlmekhlafiGHALEB A. AlmekhlafiAinda não há avaliações
- The Endocrine SystemDocumento24 páginasThe Endocrine System속강대Ainda não há avaliações
- Introduction To IridologyDocumento49 páginasIntroduction To IridologyMichael Roughan86% (7)
- Innate Immunity (DrWahyuni)Documento42 páginasInnate Immunity (DrWahyuni)Nurfadilah Zahratul WahidahAinda não há avaliações
- Chapter 35Documento4 páginasChapter 35WAHDALENA WAHIDINAinda não há avaliações
- Pex 03 02Documento5 páginasPex 03 02Jila Hafizi100% (1)
- Pathophysiology of HypovolemiaDocumento1 páginaPathophysiology of HypovolemiaSheana TmplAinda não há avaliações
- Function of KidneyDocumento66 páginasFunction of KidneyNilesh100% (4)
- Anatomy and PhysiologyDocumento2 páginasAnatomy and PhysiologyKamille Jeane Stice CavalidaAinda não há avaliações
- Animal Structure and FunctionDocumento49 páginasAnimal Structure and FunctionJohn Steven AalaAinda não há avaliações
- KokichDocumento6 páginasKokichJoy ChangAinda não há avaliações
- Article 009Documento9 páginasArticle 009MedstudAinda não há avaliações
- The Temporomandibular Joint, Part II (Myofascial Techniques)Documento4 páginasThe Temporomandibular Joint, Part II (Myofascial Techniques)Advanced-Trainings.com100% (3)
- Pex 03 03Documento7 páginasPex 03 03Jila Hafizi100% (1)
- 2020.03.10 AddendumDocumento2 páginas2020.03.10 AddendumStib BrionesAinda não há avaliações
- Dr. Tiago ScopelDocumento19 páginasDr. Tiago ScopelDr. Tiago ScopelAinda não há avaliações
- Problem-Based Learning ReportDocumento24 páginasProblem-Based Learning Reporterdayu86Ainda não há avaliações
- High-Yield Histopathology 2e PDFDocumento346 páginasHigh-Yield Histopathology 2e PDFmary100% (1)