Você também pode gostar
- Cardionursing 110207023802 Phpapp01Documento18 páginasCardionursing 110207023802 Phpapp01LudwigJayBarayuga100% (5)
- Cardiovascular SystemDocumento101 páginasCardiovascular SystemBanessa Mae GarcianoAinda não há avaliações
- Cardiovascular System BSN 1Documento16 páginasCardiovascular System BSN 1Arianne Jen GenotivaAinda não há avaliações
- Pedrajeta-Heart and Neck Vessels AssessmentDocumento4 páginasPedrajeta-Heart and Neck Vessels AssessmentAndrei PedrajetaAinda não há avaliações
- Heart Anatomy: LocationDocumento45 páginasHeart Anatomy: LocationZaira100% (1)
- Anatomy and Physiology of The Heart: Dr. N. PraveenDocumento56 páginasAnatomy and Physiology of The Heart: Dr. N. Praveenamjad khan100% (1)
- The Heart PDFDocumento13 páginasThe Heart PDFMary Ann SacramentoAinda não há avaliações
- Cardio Notes 1Documento8 páginasCardio Notes 1Lindsay Grace MandarioAinda não há avaliações
- Case 1 ObsDocumento31 páginasCase 1 ObsMatheesha HerathAinda não há avaliações
- Cardiac Anatomy, Physiology, and Cardiac Cycle: Ayu Puspita SariDocumento42 páginasCardiac Anatomy, Physiology, and Cardiac Cycle: Ayu Puspita SariAyu PuspitaAinda não há avaliações
- Cardionursing 110207023802 Phpapp01Documento18 páginasCardionursing 110207023802 Phpapp01arvinnnnAinda não há avaliações
- Transport System: Biology Unit (12/13) Kedah Matriculation CollegeDocumento26 páginasTransport System: Biology Unit (12/13) Kedah Matriculation CollegegajenraoAinda não há avaliações
- Anatomy and Physiology of The Cardiovascular System Medical Surgical NursingDocumento68 páginasAnatomy and Physiology of The Cardiovascular System Medical Surgical NursingFelix NjakeAinda não há avaliações
- The Equine Cardiovascular SystemDocumento5 páginasThe Equine Cardiovascular SystemSavannah Simone PetrachenkoAinda não há avaliações
- Cadiac Cycle, Heart Sound, ECG, HypertensionDocumento110 páginasCadiac Cycle, Heart Sound, ECG, HypertensionNilesh100% (1)
- Fisiologi Cardiovaskular and Anestesi: Boby Suryawan, S.Ked Fadilla Octovini, S.KedDocumento28 páginasFisiologi Cardiovaskular and Anestesi: Boby Suryawan, S.Ked Fadilla Octovini, S.KedBobby S PromondoAinda não há avaliações
- The Heart: Basis of Life .?Documento94 páginasThe Heart: Basis of Life .?Diksha AgrawalAinda não há avaliações
- CVS 2Documento153 páginasCVS 2khalidtalal8000Ainda não há avaliações
- Anatomy & Physiology of Heart: BY: Mr. Anurag Lecturer College of Nursing DMC & H, LudhianaDocumento56 páginasAnatomy & Physiology of Heart: BY: Mr. Anurag Lecturer College of Nursing DMC & H, Ludhianapreet kaurAinda não há avaliações
- Sistem Kardiovaskular: Cardiac Output Dan Otot JantungDocumento46 páginasSistem Kardiovaskular: Cardiac Output Dan Otot JantungSusanna Arie KAinda não há avaliações
- Cardiogenic ShockDocumento14 páginasCardiogenic ShockZellanien hdAinda não há avaliações
- WK 1& 2 LectureDocumento149 páginasWK 1& 2 LectureElma SekikorolevuAinda não há avaliações
- The HeartDocumento13 páginasThe HeartMary Ann SacramentoAinda não há avaliações
- NPTE CArdio NotesDocumento27 páginasNPTE CArdio NotesAubrey Vale SagunAinda não há avaliações
- Cardiology: DR Isaak M Osman MBCHB, Mmed Int. Medicine/Cardiology 10 Sept 2019Documento19 páginasCardiology: DR Isaak M Osman MBCHB, Mmed Int. Medicine/Cardiology 10 Sept 2019Imraan MohaAinda não há avaliações
- Cardiovascular SystemDocumento34 páginasCardiovascular Systemurooj100% (1)
- Anatomy of The HeartDocumento7 páginasAnatomy of The HeartJanice ScatesAinda não há avaliações
- 2015A&PIntro CardiovascularHandoutDocumento16 páginas2015A&PIntro CardiovascularHandoutMaggieHameedAinda não há avaliações
- Anatomy & Physiology NotesDocumento56 páginasAnatomy & Physiology NotesChristina Gonez100% (2)
- Cardiovascular SystemDocumento12 páginasCardiovascular SystemDevendra RawatAinda não há avaliações
- Cardiovascular Physiology and Anethesia: Boby Suryawan, S.Ked Fadilla Octovini, S.KedDocumento34 páginasCardiovascular Physiology and Anethesia: Boby Suryawan, S.Ked Fadilla Octovini, S.KedBobby S PromondoAinda não há avaliações
- CardiovascularDocumento6 páginasCardiovascularMabes100% (1)
- Chapter 19 Heart Marie BDocumento29 páginasChapter 19 Heart Marie BomarAinda não há avaliações
- Chapter 20 Heart and Neck VesselsDocumento10 páginasChapter 20 Heart and Neck Vesselsannoja selvaAinda não há avaliações
- Module Cardiovascular System Anatomy and PhysiologyDocumento9 páginasModule Cardiovascular System Anatomy and PhysiologyPATRICIA KAYE RIOAinda não há avaliações
- The HeartDocumento65 páginasThe HeartMichael SamaniegoAinda não há avaliações
- EKG Study Guide RevisedDocumento29 páginasEKG Study Guide Revisedflashyboy506Ainda não há avaliações
- Cardiovascular System: Presented by DR Aparna Ramachandran Mds 1 Dept of Public Health DentistryDocumento73 páginasCardiovascular System: Presented by DR Aparna Ramachandran Mds 1 Dept of Public Health DentistryAparna RamachandranAinda não há avaliações
- Lec 4Documento59 páginasLec 4علي صفاء عبد الزهرهAinda não há avaliações
- Circulatory SystemDocumento25 páginasCirculatory SystemadnanAinda não há avaliações
- The Equine Cardiovascular SystemDocumento7 páginasThe Equine Cardiovascular SystemSavannah Simone PetrachenkoAinda não há avaliações
- Cardiovascular and Syrculation System, 2013Documento92 páginasCardiovascular and Syrculation System, 2013Santi Purnama SariAinda não há avaliações
- Salcedo ANPH111 The Cardiovascular System23Documento46 páginasSalcedo ANPH111 The Cardiovascular System23ajline.esto23Ainda não há avaliações
- Cardiovascular System: Dr. Mohanad R. AlwanDocumento46 páginasCardiovascular System: Dr. Mohanad R. Alwanmohanad11Ainda não há avaliações
- Cardio SlidesDocumento309 páginasCardio SlidesGina VasquezAinda não há avaliações
- Cardiovascular System: Blood VesselsDocumento12 páginasCardiovascular System: Blood VesselsSoniyaJI84100% (1)
- Heart and CirculationDocumento63 páginasHeart and CirculationNuraina SakinaAinda não há avaliações
- Medical Terminology Cardiovascular SystemDocumento35 páginasMedical Terminology Cardiovascular Systemapi-26819951486% (7)
- HeartDocumento36 páginasHeartSoovendran VaradarajanAinda não há avaliações
- The Cardiovascular System: Click To Edit Master Subtitle StyleDocumento65 páginasThe Cardiovascular System: Click To Edit Master Subtitle StyleBien EstrellaAinda não há avaliações
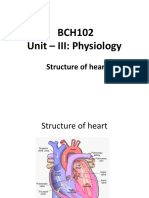
- BCH102 Unit - III: Physiology: Structure of HeartDocumento17 páginasBCH102 Unit - III: Physiology: Structure of Heartdivya vajpayeeAinda não há avaliações
- Components of The Cardiovascular SystemDocumento23 páginasComponents of The Cardiovascular SystemMr. DummyAinda não há avaliações
- Cardiovascular SystemDocumento14 páginasCardiovascular SystemAthena Huynh100% (1)
- 2014 Kuliah Fisiologi JantungDocumento102 páginas2014 Kuliah Fisiologi JantungAlfia NadiraAinda não há avaliações
- Anatomy and Physiology of The HeartDocumento21 páginasAnatomy and Physiology of The HeartNina OaipAinda não há avaliações
- Hemodinamik Pada Sistem Kardiovaskuler - PPTDocumento114 páginasHemodinamik Pada Sistem Kardiovaskuler - PPTIsna ZalwaAinda não há avaliações
- Ila College of Health Kuje: Cardiovascular SystemDocumento24 páginasIla College of Health Kuje: Cardiovascular SystemDaniel DendaAinda não há avaliações
- 81: Mammalian Heart and Its RegulationDocumento75 páginas81: Mammalian Heart and Its RegulationIt's Ika100% (1)
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideAinda não há avaliações
- Daftar PustakaDocumento7 páginasDaftar PustakaAndra HijratulAinda não há avaliações
- Accordion Sign-Appearance (C. Difficile)Documento41 páginasAccordion Sign-Appearance (C. Difficile)Andra HijratulAinda não há avaliações
- For Bitcoin UsersDocumento1 páginaFor Bitcoin UsersAndra HijratulAinda não há avaliações
- Accordion Sign-Appearance (C. Difficile)Documento41 páginasAccordion Sign-Appearance (C. Difficile)Andra HijratulAinda não há avaliações
- Marco Conceptual para La AcciónDocumento79 páginasMarco Conceptual para La AcciónJessica Mac DonaldAinda não há avaliações
- Get My All Downloads From HereDocumento1 páginaGet My All Downloads From HereAndra Hijratul100% (1)
- I Do NOT Release These Programs So That YouDocumento3 páginasI Do NOT Release These Programs So That YouPhearun PayAinda não há avaliações
- RMS UsgDocumento13 páginasRMS UsgAndra HijratulAinda não há avaliações
- Cardiac Output, Blood Flow, and Blood PressureDocumento74 páginasCardiac Output, Blood Flow, and Blood PressureAndra HijratulAinda não há avaliações
- Human Body: Circulatory SystemDocumento46 páginasHuman Body: Circulatory SystemAndra HijratulAinda não há avaliações
- DR/ Abd Allah Nazeer. MD.: Radiological Vascular Anatomy of The Upper and Lower LimbsDocumento80 páginasDR/ Abd Allah Nazeer. MD.: Radiological Vascular Anatomy of The Upper and Lower LimbsAndra HijratulAinda não há avaliações
- Anatomyofcarduacsystem-181124055746 2Documento91 páginasAnatomyofcarduacsystem-181124055746 2Andra HijratulAinda não há avaliações
- Organizational Structure: Mintzberg's Framework: Fred C. LunenburgDocumento14 páginasOrganizational Structure: Mintzberg's Framework: Fred C. LunenburgAndra HijratulAinda não há avaliações
- Organizational Structure: Mintzberg's Framework: Fred C. LunenburgDocumento14 páginasOrganizational Structure: Mintzberg's Framework: Fred C. LunenburgAndra HijratulAinda não há avaliações
- Hellp SindromeDocumento24 páginasHellp SindromeAndra HijratulAinda não há avaliações
- DEPKES RI NEW Pedoman Nasional Penanggulangan TBC 2011Documento110 páginasDEPKES RI NEW Pedoman Nasional Penanggulangan TBC 2011familyman8091% (11)
- DEPKES RI NEW Pedoman Nasional Penanggulangan TBC 2011Documento110 páginasDEPKES RI NEW Pedoman Nasional Penanggulangan TBC 2011familyman8091% (11)
- LWW Bates Osce1 Chestpain Transcript FinalDocumento6 páginasLWW Bates Osce1 Chestpain Transcript FinalFuego151Ainda não há avaliações
- Abnormal Heart Sounds: First Heart Sound (S)Documento4 páginasAbnormal Heart Sounds: First Heart Sound (S)Faris Mufid MadyaputraAinda não há avaliações
- Health Assessment Lesson 1Documento44 páginasHealth Assessment Lesson 1Bernice EbbiAinda não há avaliações
- #3 Clinical - Examination 101-150Documento50 páginas#3 Clinical - Examination 101-150z zzAinda não há avaliações
- Heart Failure Nursing Care Plans - 15 Nursing Diagnosis - NurseslabsDocumento13 páginasHeart Failure Nursing Care Plans - 15 Nursing Diagnosis - NurseslabsJOSHUA DICHOSOAinda não há avaliações
- Biomedical InstrumentationDocumento13 páginasBiomedical InstrumentationNisha ManiAinda não há avaliações
- HEART MURMURS by NISHDocumento41 páginasHEART MURMURS by NISHurtikikeAinda não há avaliações
- 1800 MCQ Revised VersionDocumento606 páginas1800 MCQ Revised VersionFarah FarahAinda não há avaliações
- Physiological Changes During PregnancyDocumento38 páginasPhysiological Changes During PregnancyHei KamuAinda não há avaliações
- Cardiac Cycle WorksheetDocumento10 páginasCardiac Cycle WorksheetRamesh Kumar MuniandyAinda não há avaliações
- Nbme Test Taking StrategiesDocumento13 páginasNbme Test Taking StrategiesSunita Shah0% (1)
- Step 1 ShartzDocumento333 páginasStep 1 ShartzDaniella Vazquez100% (1)
- CARDIOVASCULAR ASSESSMENT NotesDocumento6 páginasCARDIOVASCULAR ASSESSMENT NotesJunry PilapilAinda não há avaliações
- Anatomy and Physiology ASCVDDocumento9 páginasAnatomy and Physiology ASCVDAlvheen JoaquinAinda não há avaliações
- Head To Toe Assessment - InserviceDocumento10 páginasHead To Toe Assessment - InservicelovelivetaylorAinda não há avaliações
- NU632 Unit 4 Discussion CaseDocumento2 páginasNU632 Unit 4 Discussion CaseMaria Ines OrtizAinda não há avaliações
- Guide To Paediatric Clinical Examination (24 PGS)Documento24 páginasGuide To Paediatric Clinical Examination (24 PGS)Shre RanjithamAinda não há avaliações
- Preskas Hypoxic Spell Patofisiologi Dan ManajemenDocumento22 páginasPreskas Hypoxic Spell Patofisiologi Dan Manajemensurya marthiasAinda não há avaliações
- Collecting Objective DataDocumento61 páginasCollecting Objective DataAdrianAripAinda não há avaliações
- MS Practice Questions With RationaleDocumento13 páginasMS Practice Questions With RationaleRey Gil Flee GabonadaAinda não há avaliações
- Test Bank CardioDocumento16 páginasTest Bank CardioLudwigJayBarayuga86% (7)
- CardioDocumento146 páginasCardiobbdddAinda não há avaliações
- Physiology of The Cardiovascular System-CVSDocumento56 páginasPhysiology of The Cardiovascular System-CVSAmanuel MaruAinda não há avaliações
- Heart SoundsDocumento17 páginasHeart SoundsAlfrin Antony100% (3)
- JARVIS Exam #4 Health AssessmentDocumento24 páginasJARVIS Exam #4 Health AssessmentCTuag100% (3)
- Physical Examination of CVDocumento40 páginasPhysical Examination of CVNur Hikmah KusumaAinda não há avaliações
- Biopac Lesson 17 ProcedureDocumento16 páginasBiopac Lesson 17 ProcedureEdwin PurcellAinda não há avaliações
- Skenario 2Documento3 páginasSkenario 2emalliaAinda não há avaliações
- Problem StatementDocumento18 páginasProblem StatementvmrekhateAinda não há avaliações