Você também pode gostar
- Exit Interview QuestionsDocumento3 páginasExit Interview Questionsapi-371785797Ainda não há avaliações
- Apta Membership CertificateDocumento1 páginaApta Membership Certificateapi-371785797Ainda não há avaliações
- Gradereport 1Documento1 páginaGradereport 1api-371785797Ainda não há avaliações
- Mental Health Conference Series Cognitive and Behavioral Sequelae of Covid-19 InfectionDocumento1 páginaMental Health Conference Series Cognitive and Behavioral Sequelae of Covid-19 Infectionapi-371785797Ainda não há avaliações
- Interdisciplinary Project - OsantowskiDocumento6 páginasInterdisciplinary Project - Osantowskiapi-371785797Ainda não há avaliações
- Gradereport 5Documento1 páginaGradereport 5api-371785797Ainda não há avaliações
- Gradereport 2019-20 SummerDocumento1 páginaGradereport 2019-20 Summerapi-468018392Ainda não há avaliações
- Case Report 1 Final Draft 12Documento65 páginasCase Report 1 Final Draft 12api-371785797Ainda não há avaliações
- GradereportDocumento1 páginaGradereportapi-371785797Ainda não há avaliações
- Post Print Score ReportDocumento1 páginaPost Print Score Reportapi-371785797Ainda não há avaliações
- Esophageal Cancer InserviceDocumento18 páginasEsophageal Cancer Inserviceapi-371785797Ainda não há avaliações
- Group PresentationDocumento13 páginasGroup Presentationapi-371785797Ainda não há avaliações
- Gradereport 2Documento1 páginaGradereport 2api-371785797Ainda não há avaliações
- Self Assessment - Second Year 2019-2020Documento4 páginasSelf Assessment - Second Year 2019-2020api-371785797Ainda não há avaliações
- Part 1 Task A Field Observation - OsantowskiDocumento6 páginasPart 1 Task A Field Observation - Osantowskiapi-371785797Ainda não há avaliações
- Reflective JournalDocumento26 páginasReflective Journalapi-371785797Ainda não há avaliações
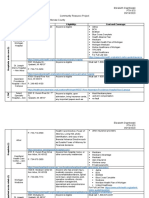
- Community Resource ProjectDocumento9 páginasCommunity Resource Projectapi-371785797Ainda não há avaliações
- Gradereport 3Documento1 páginaGradereport 3api-371785797Ainda não há avaliações
- Osantowski Rolling-Teaching Activity Paper 1Documento11 páginasOsantowski Rolling-Teaching Activity Paper 1api-371785797Ainda não há avaliações
- Greatest Moment Slide - Osantowski and SlocumDocumento1 páginaGreatest Moment Slide - Osantowski and Slocumapi-371785797Ainda não há avaliações
- GradereportDocumento1 páginaGradereportapi-467445554Ainda não há avaliações
- Final Ethics Paper - OsantowskiDocumento10 páginasFinal Ethics Paper - Osantowskiapi-371785797Ainda não há avaliações
- Jennifer Exercise ListDocumento1 páginaJennifer Exercise Listapi-371785797Ainda não há avaliações
- Citi - OsantowskiDocumento1 páginaCiti - Osantowskiapi-371785797Ainda não há avaliações
- Updated Game PlanDocumento3 páginasUpdated Game Planapi-371785797Ainda não há avaliações
- Ptso Certification 2018-2019Documento1 páginaPtso Certification 2018-2019api-371785797Ainda não há avaliações
- Case Report - Osantowski and AyacheDocumento14 páginasCase Report - Osantowski and Ayacheapi-371785797Ainda não há avaliações
- Osantowski Pre 2019 2Documento7 páginasOsantowski Pre 2019 2api-371785797Ainda não há avaliações
- Ptso Leadership 2018-2019Documento1 páginaPtso Leadership 2018-2019api-371785797Ainda não há avaliações
- Exam 4 Study Guide - Eo JTZDocumento16 páginasExam 4 Study Guide - Eo JTZapi-371785797Ainda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Manila Pilots Association Immune from Attachment for Member's DebtDocumento2 páginasManila Pilots Association Immune from Attachment for Member's DebtAngelic ArcherAinda não há avaliações
- Classen 2012 - Rural Space in The Middle Ages and Early Modern Age-De Gruyter (2012)Documento932 páginasClassen 2012 - Rural Space in The Middle Ages and Early Modern Age-De Gruyter (2012)maletrejoAinda não há avaliações
- Sigma Chi Foundation - 2016 Annual ReportDocumento35 páginasSigma Chi Foundation - 2016 Annual ReportWes HoltsclawAinda não há avaliações
- List of Parts For Diy Dremel CNC by Nikodem Bartnik: Part Name Quantity BanggoodDocumento6 páginasList of Parts For Diy Dremel CNC by Nikodem Bartnik: Part Name Quantity Banggoodyogesh parmarAinda não há avaliações
- How To Use This Engine Repair Manual: General InformationDocumento3 páginasHow To Use This Engine Repair Manual: General InformationHenry SilvaAinda não há avaliações
- 1 - Nature and Dev - Intl LawDocumento20 páginas1 - Nature and Dev - Intl Lawaditya singhAinda não há avaliações
- Page 17 - Word Connection, LiaisonsDocumento2 páginasPage 17 - Word Connection, Liaisonsstarskyhutch0% (1)
- Excel Keyboard Shortcuts MasterclassDocumento18 páginasExcel Keyboard Shortcuts MasterclassluinksAinda não há avaliações
- Chapter 12 The Incredible Story of How The Great Controversy Was Copied by White From Others, and Then She Claimed It To Be Inspired.Documento6 páginasChapter 12 The Incredible Story of How The Great Controversy Was Copied by White From Others, and Then She Claimed It To Be Inspired.Barry Lutz Sr.Ainda não há avaliações
- Kedudukan Dan Fungsi Pembukaan Undang-Undang Dasar 1945: Pembelajaran Dari Tren GlobalDocumento20 páginasKedudukan Dan Fungsi Pembukaan Undang-Undang Dasar 1945: Pembelajaran Dari Tren GlobalRaissa OwenaAinda não há avaliações
- Advanced VLSI Architecture Design For Emerging Digital SystemsDocumento78 páginasAdvanced VLSI Architecture Design For Emerging Digital Systemsgangavinodc123Ainda não há avaliações
- Midgard - Player's Guide To The Seven Cities PDFDocumento32 páginasMidgard - Player's Guide To The Seven Cities PDFColin Khoo100% (8)
- Apple NotesDocumento3 páginasApple NotesKrishna Mohan ChennareddyAinda não há avaliações
- Ten - Doc. TR 20 01 (Vol. II)Documento309 páginasTen - Doc. TR 20 01 (Vol. II)Manoj OjhaAinda não há avaliações
- Group 9 - LLIR ProjectDocumento8 páginasGroup 9 - LLIR ProjectRahul RaoAinda não há avaliações
- IB Theatre: The Ilussion of InclusionDocumento15 páginasIB Theatre: The Ilussion of InclusionLazar LukacAinda não há avaliações
- UG022510 International GCSE in Business Studies 4BS0 For WebDocumento57 páginasUG022510 International GCSE in Business Studies 4BS0 For WebAnonymous 8aj9gk7GCLAinda não há avaliações
- HERMAgreenGuide EN 01Documento4 páginasHERMAgreenGuide EN 01PaulAinda não há avaliações
- Environmental Science PDFDocumento118 páginasEnvironmental Science PDFJieyan OliverosAinda não há avaliações
- Brain Chip ReportDocumento30 páginasBrain Chip Reportsrikanthkalemla100% (3)
- Topic 1 in 21st CneturyDocumento8 páginasTopic 1 in 21st CneturyLuwisa RamosAinda não há avaliações
- Get 1. Verb Gets, Getting Past Got Past Participle Got, GottenDocumento2 páginasGet 1. Verb Gets, Getting Past Got Past Participle Got, GottenOlga KardashAinda não há avaliações
- Episode 8Documento11 páginasEpisode 8annieguillermaAinda não há avaliações
- Clinical Eval Brittany RivasDocumento8 páginasClinical Eval Brittany Rivasapi-613460741Ainda não há avaliações
- 14 Jet Mykles - Heaven Sent 5 - GenesisDocumento124 páginas14 Jet Mykles - Heaven Sent 5 - Genesiskeikey2050% (2)
- 5 6107116501871886934Documento38 páginas5 6107116501871886934Harsha VardhanAinda não há avaliações
- ISA standards, materials, and control room conceptsDocumento8 páginasISA standards, materials, and control room conceptsGiovanniAinda não há avaliações
- Ethnic Conflicts and PeacekeepingDocumento2 páginasEthnic Conflicts and PeacekeepingAmna KhanAinda não há avaliações
- Markle 1999 Shield VeriaDocumento37 páginasMarkle 1999 Shield VeriaMads Sondre PrøitzAinda não há avaliações
- 11th AccountancyDocumento13 páginas11th AccountancyNarendar KumarAinda não há avaliações