Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Key Points/: Study GuideDocumento48 páginasKey Points/: Study Guidedanni100% (1)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- HSS - Summer 2020 - Syllabus - ANTH 1667Documento7 páginasHSS - Summer 2020 - Syllabus - ANTH 1667Bruce JobseAinda não há avaliações
- HSS - Summer 2020 - Syllabus - ANTH 1667Documento7 páginasHSS - Summer 2020 - Syllabus - ANTH 1667Bruce JobseAinda não há avaliações
- Indwelling Urinary Catheterization 1Documento5 páginasIndwelling Urinary Catheterization 1Mercy Anne EcatAinda não há avaliações
- Scotchcast PDFDocumento311 páginasScotchcast PDFSaadAinda não há avaliações
- A Year of Blessings: Regina Coeli ReportDocumento12 páginasA Year of Blessings: Regina Coeli ReportBruce JobseAinda não há avaliações
- Metal Gods: Dominic Covey Chris DavisDocumento66 páginasMetal Gods: Dominic Covey Chris DavisBruce JobseAinda não há avaliações
- Fuel Cell Handbook (2000)Documento352 páginasFuel Cell Handbook (2000)erhan ünal100% (4)
- Charles Rice: Cover: EditingDocumento11 páginasCharles Rice: Cover: EditingBruce JobseAinda não há avaliações
- RPO0100b 25Documento130 páginasRPO0100b 25Bruce JobseAinda não há avaliações
- Remington II00 SystemDocumento78 páginasRemington II00 SystemBruce JobseAinda não há avaliações
- Phoenix Command Panzer WWII Medium TanksDocumento32 páginasPhoenix Command Panzer WWII Medium TanksBruce Jobse100% (1)
- Prevalence and Outcomes in Patients Undergoing Reintubation After Anterior Cervical Spine Surgery - Results From AOSpine North America MultiCenter Study On 8887 PatientsDocumento7 páginasPrevalence and Outcomes in Patients Undergoing Reintubation After Anterior Cervical Spine Surgery - Results From AOSpine North America MultiCenter Study On 8887 PatientsBruce JobseAinda não há avaliações
- Vexilliod Tabloid - 73Documento12 páginasVexilliod Tabloid - 73Bruce JobseAinda não há avaliações
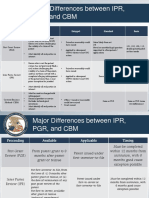
- Major Differences Between IPR, PGR, and CBM: Inter Partes Review (IPR) Petitioner Estoppel Standard BasisDocumento2 páginasMajor Differences Between IPR, PGR, and CBM: Inter Partes Review (IPR) Petitioner Estoppel Standard BasisBruce JobseAinda não há avaliações
- AOSpine Global Spine Journal Vol 7 (1S) 46S-52SDocumento7 páginasAOSpine Global Spine Journal Vol 7 (1S) 46S-52SBruce JobseAinda não há avaliações
- Kan 2019 RDF Events and Nonevetns PDFDocumento14 páginasKan 2019 RDF Events and Nonevetns PDFBruce JobseAinda não há avaliações
- Freeway Warrior 02 PDFDocumento301 páginasFreeway Warrior 02 PDFBruce Jobse100% (1)
- C5 Palsy After Cervical Spine Surgery - A Multicenter Retrospective Review of 59 CasesDocumento7 páginasC5 Palsy After Cervical Spine Surgery - A Multicenter Retrospective Review of 59 CasesBruce JobseAinda não há avaliações
- A Multicenter Study of The Presentation, Treatment, and Outcomes of Cervical Dural TearsDocumento6 páginasA Multicenter Study of The Presentation, Treatment, and Outcomes of Cervical Dural TearsBruce JobseAinda não há avaliações
- AOSpine Global Spine Journal Vol 7 (1S) 46S-52SDocumento7 páginasAOSpine Global Spine Journal Vol 7 (1S) 46S-52SBruce JobseAinda não há avaliações
- Firearms Oicw Multipurpose Weapon Us Patent 6250194Documento17 páginasFirearms Oicw Multipurpose Weapon Us Patent 6250194jim100abAinda não há avaliações
- Freeway Warrior 03 PDFDocumento323 páginasFreeway Warrior 03 PDFBruce JobseAinda não há avaliações
- Freeway Warrior 01Documento291 páginasFreeway Warrior 01Bruce JobseAinda não há avaliações
- Army - tc90 1 - Training For Urban OperationsDocumento149 páginasArmy - tc90 1 - Training For Urban OperationsMeowmix100% (6)
- CP CommentaryDocumento2 páginasCP Commentarykaan_yagmur7711Ainda não há avaliações
- Pilon Fractures Preventing ComplicationsDocumento12 páginasPilon Fractures Preventing ComplicationsjojoAinda não há avaliações
- Surgical Management of Traumatic Brain InjuryDocumento41 páginasSurgical Management of Traumatic Brain InjuryAkreditasi Sungai AbangAinda não há avaliações
- Ripperologist 73Documento75 páginasRipperologist 73CustardScreamAinda não há avaliações
- OutlineDocumento3 páginasOutlineapi-551638506Ainda não há avaliações
- Massive Hemorrhage ProtocolDocumento19 páginasMassive Hemorrhage ProtocolYeseniaAinda não há avaliações
- Dr. Risma Dikirim Pukul 0 16sympo OptimizingDocumento30 páginasDr. Risma Dikirim Pukul 0 16sympo OptimizingAlthof SonaAinda não há avaliações
- Cardiopulmonary AssessmentDocumento22 páginasCardiopulmonary AssessmentMandeep Jangra100% (1)
- Revision Tables - 270820162807Documento105 páginasRevision Tables - 270820162807flickers xxxAinda não há avaliações
- Advanced Heart Failure: A Position Statementof The Heart Failure Association of Theeuropean Society of CardiologyDocumento11 páginasAdvanced Heart Failure: A Position Statementof The Heart Failure Association of Theeuropean Society of CardiologyFlorentino Remon GodoyAinda não há avaliações
- 812-Article Text-2928-1-10-20191129 (PMR)Documento6 páginas812-Article Text-2928-1-10-20191129 (PMR)Azza SintaAinda não há avaliações
- Nursing ICUDocumento2 páginasNursing ICUKomal Tomar50% (2)
- Abstract No. 301 - Angiographic Catheters - A Comprehensive Review For The Interventionalist In-TrainingDocumento2 páginasAbstract No. 301 - Angiographic Catheters - A Comprehensive Review For The Interventionalist In-TrainingPeter LiAinda não há avaliações
- Osteology of Skull & Vertebral ColumnDocumento93 páginasOsteology of Skull & Vertebral ColumnElisa NAinda não há avaliações
- CH 071 Acute Kidney Injury in ChildrenDocumento9 páginasCH 071 Acute Kidney Injury in Childrenarun babuAinda não há avaliações
- Running SuturesDocumento3 páginasRunning SuturesIo DobriAinda não há avaliações
- Umbilical Artery CatheterizationDocumento9 páginasUmbilical Artery CatheterizationrohitAinda não há avaliações
- NCM118 Keynote - Docx 1Documento40 páginasNCM118 Keynote - Docx 1JINYVEV APARICIAinda não há avaliações
- Humerus Anterolateral ApproachDocumento15 páginasHumerus Anterolateral ApproachHussein SamhatAinda não há avaliações
- Volume 2, Issue 3Documento152 páginasVolume 2, Issue 3Asfandyar Sheikh75% (4)
- Medical Treatment of Battle WoundsDocumento6 páginasMedical Treatment of Battle Woundskatgirl999Ainda não há avaliações
- Cabg 130102113345 Phpapp01Documento29 páginasCabg 130102113345 Phpapp01md.dascalescu2486Ainda não há avaliações
- ECG WorksheetDocumento4 páginasECG WorksheetNikki GuisonAinda não há avaliações
- Radiology: Textbook ofDocumento16 páginasRadiology: Textbook ofthsisbolt02Ainda não há avaliações
- Knee Joint Anatomy ManualDocumento6 páginasKnee Joint Anatomy ManualDungani AllanAinda não há avaliações
- Perfusionist Job DescriptionDocumento3 páginasPerfusionist Job DescriptionNouman IshaqAinda não há avaliações
- MAPCA'sDocumento1 páginaMAPCA'sFania Dora AslamyAinda não há avaliações