Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- NOP PortalDocumento87 páginasNOP PortalCarlos RicoAinda não há avaliações
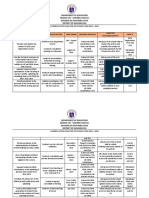
- Action Plan Lis 2021-2022Documento3 páginasAction Plan Lis 2021-2022Vervie BingalogAinda não há avaliações
- Experiment On Heat Transfer Through Fins Having Different NotchesDocumento4 páginasExperiment On Heat Transfer Through Fins Having Different NotcheskrantiAinda não há avaliações
- Analysis of Material Nonlinear Problems Using Pseudo-Elastic Finite Element MethodDocumento5 páginasAnalysis of Material Nonlinear Problems Using Pseudo-Elastic Finite Element MethodleksremeshAinda não há avaliações
- Basic Vibration Analysis Training-1Documento193 páginasBasic Vibration Analysis Training-1Sanjeevi Kumar SpAinda não há avaliações
- CIR Vs PAL - ConstructionDocumento8 páginasCIR Vs PAL - ConstructionEvan NervezaAinda não há avaliações
- POST TEST 3 and POST 4, in ModuleDocumento12 páginasPOST TEST 3 and POST 4, in ModuleReggie Alis100% (1)
- Privacy: Based On Slides Prepared by Cyndi Chie, Sarah Frye and Sharon Gray. Fifth Edition Updated by Timothy HenryDocumento50 páginasPrivacy: Based On Slides Prepared by Cyndi Chie, Sarah Frye and Sharon Gray. Fifth Edition Updated by Timothy HenryAbid KhanAinda não há avaliações
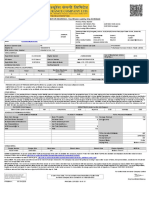
- MOTOR INSURANCE - Two Wheeler Liability Only SCHEDULEDocumento1 páginaMOTOR INSURANCE - Two Wheeler Liability Only SCHEDULESuhail V VAinda não há avaliações
- Microwave Drying of Gelatin Membranes and Dried Product Properties CharacterizationDocumento28 páginasMicrowave Drying of Gelatin Membranes and Dried Product Properties CharacterizationDominico Delven YapinskiAinda não há avaliações
- Food and Beverage Department Job DescriptionDocumento21 páginasFood and Beverage Department Job DescriptionShergie Rivera71% (7)
- Instructions For Microsoft Teams Live Events: Plan and Schedule A Live Event in TeamsDocumento9 páginasInstructions For Microsoft Teams Live Events: Plan and Schedule A Live Event in TeamsAnders LaursenAinda não há avaliações
- STM - Welding BookDocumento5 páginasSTM - Welding BookAlvin MoollenAinda não há avaliações
- Online EarningsDocumento3 páginasOnline EarningsafzalalibahttiAinda não há avaliações
- FIRE FIGHTING ROBOT (Mini Project)Documento21 páginasFIRE FIGHTING ROBOT (Mini Project)Hisham Kunjumuhammed100% (2)
- Rofi Operation and Maintenance ManualDocumento3 páginasRofi Operation and Maintenance ManualSteve NewmanAinda não há avaliações
- Aircraftdesigngroup PDFDocumento1 páginaAircraftdesigngroup PDFsugiAinda não há avaliações
- Termination LetterDocumento2 páginasTermination Letterultakam100% (1)
- QUIZ Group 1 Answer KeyDocumento3 páginasQUIZ Group 1 Answer KeyJames MercadoAinda não há avaliações
- Government of West Bengal Finance (Audit) Department: NABANNA', HOWRAH-711102 No. Dated, The 13 May, 2020Documento2 páginasGovernment of West Bengal Finance (Audit) Department: NABANNA', HOWRAH-711102 No. Dated, The 13 May, 2020Satyaki Prasad MaitiAinda não há avaliações
- Amerisolar AS 7M144 HC Module Specification - CompressedDocumento2 páginasAmerisolar AS 7M144 HC Module Specification - CompressedMarcus AlbaniAinda não há avaliações
- Activity Description Predecessor Time (Days) Activity Description Predecessor ADocumento4 páginasActivity Description Predecessor Time (Days) Activity Description Predecessor AAlvin LuisaAinda não há avaliações
- Fernando Salgado-Hernandez, A206 263 000 (BIA June 7, 2016)Documento7 páginasFernando Salgado-Hernandez, A206 263 000 (BIA June 7, 2016)Immigrant & Refugee Appellate Center, LLCAinda não há avaliações
- RENCANA KERJA Serious Inspeksi#3 Maret-April 2019Documento2 páginasRENCANA KERJA Serious Inspeksi#3 Maret-April 2019Nur Ali SaidAinda não há avaliações
- Himachal Pradesh Important NumbersDocumento3 páginasHimachal Pradesh Important NumbersRaghav RahinwalAinda não há avaliações
- 21st Bomber Command Tactical Mission Report 178, OcrDocumento49 páginas21st Bomber Command Tactical Mission Report 178, OcrJapanAirRaidsAinda não há avaliações
- Expense Tracking - How Do I Spend My MoneyDocumento2 páginasExpense Tracking - How Do I Spend My MoneyRenata SánchezAinda não há avaliações
- Wiley Chapter 11 Depreciation Impairments and DepletionDocumento43 páginasWiley Chapter 11 Depreciation Impairments and Depletion靳雪娇Ainda não há avaliações
- Doas - MotorcycleDocumento2 páginasDoas - MotorcycleNaojAinda não há avaliações
- Basic DfwmacDocumento6 páginasBasic DfwmacDinesh Kumar PAinda não há avaliações