Você também pode gostar
- Transport of Critically Ill Adults 2011Documento1 páginaTransport of Critically Ill Adults 2011velocity25Ainda não há avaliações
- Abst 1Documento20 páginasAbst 1martyAinda não há avaliações
- Eucast Exposicion PDFDocumento20 páginasEucast Exposicion PDFJordan PuenteAinda não há avaliações
- ARP Antibiotics Currently in Global Clinical Development Data Table v2Documento10 páginasARP Antibiotics Currently in Global Clinical Development Data Table v2tanishtarun06Ainda não há avaliações
- (PIDST) - 391 - Pidst - 20111020114358 - Filejou 2Documento20 páginas(PIDST) - 391 - Pidst - 20111020114358 - Filejou 2Nareunart KongkaAinda não há avaliações
- Communicable Disease Summary: A Guide For SchoolsDocumento31 páginasCommunicable Disease Summary: A Guide For SchoolsMohamoud MohamedAinda não há avaliações
- WHO EMP MAR 2012.3 Eng PDFDocumento78 páginasWHO EMP MAR 2012.3 Eng PDFonovAinda não há avaliações
- Surgical Site Infection Due To Mycobacterium Peregrinum: A Case Report and Literature ReviewDocumento3 páginasSurgical Site Infection Due To Mycobacterium Peregrinum: A Case Report and Literature ReviewHanung PujanggaAinda não há avaliações
- Karlien Vanhouteghem, Annelies Aerssens, Dirk Ommeslag, Jerina Boelens, Steven Callens, Anne-Marie Van Den AbeeleDocumento1 páginaKarlien Vanhouteghem, Annelies Aerssens, Dirk Ommeslag, Jerina Boelens, Steven Callens, Anne-Marie Van Den AbeeleAfien MuktiAinda não há avaliações
- Questions 43-52 Are Based On The Following Passages.: Aureus and Streptococcus Pneumoniae) Were TreatedDocumento11 páginasQuestions 43-52 Are Based On The Following Passages.: Aureus and Streptococcus Pneumoniae) Were TreatedKellyAinda não há avaliações
- Study of Factors Associated With Acute PharyngitisDocumento2 páginasStudy of Factors Associated With Acute PharyngitisMicaAinda não há avaliações
- Farmakoterapi Penyakit Paru Obstruksi Kronik (PPOK) : Tinjauan PustakaDocumento10 páginasFarmakoterapi Penyakit Paru Obstruksi Kronik (PPOK) : Tinjauan PustakaLilisAinda não há avaliações
- MODULE B TBPresentation3Documento62 páginasMODULE B TBPresentation3Jerommy MalweleAinda não há avaliações
- Thu 348 Ilc2022Documento1 páginaThu 348 Ilc2022rtthrtfhAinda não há avaliações
- Booklet Antimicrobial Prescribing Educational Booklet Offered by BiomerieuxDocumento21 páginasBooklet Antimicrobial Prescribing Educational Booklet Offered by Biomerieuxeli ferraraAinda não há avaliações
- Acute Respiratory Infeciton (ARI)Documento19 páginasAcute Respiratory Infeciton (ARI)Haryo Prakoso Adhi PAinda não há avaliações
- Treatmen PharyngitisDocumento8 páginasTreatmen PharyngitismeysiskaAinda não há avaliações
- Acute Respiratory InfectionDocumento15 páginasAcute Respiratory InfectionmAinda não há avaliações
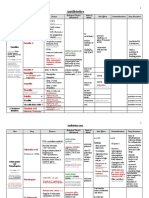
- Antimicrobial Drugs TableDocumento19 páginasAntimicrobial Drugs TableLaylee ClareAinda não há avaliações
- Cartaaleditor PUBMEDDocumento3 páginasCartaaleditor PUBMEDSandra DelgadoAinda não há avaliações
- SWORBHPPCPMedical Directive Book 2015Documento148 páginasSWORBHPPCPMedical Directive Book 2015richardphilp1640Ainda não há avaliações
- Managing Microbes Poster AIF 00612Documento1 páginaManaging Microbes Poster AIF 00612Devina Sari PratiwiAinda não há avaliações
- Medical Prevention of Recurrent Acute Otitis Media: An Updated OverviewDocumento10 páginasMedical Prevention of Recurrent Acute Otitis Media: An Updated OverviewholaAinda não há avaliações
- Real-Time Alerting System For COVID-19 and Other Stress Events Using Wearable DataDocumento26 páginasReal-Time Alerting System For COVID-19 and Other Stress Events Using Wearable DataLuiz Folha FlaskAinda não há avaliações
- Affiche Infection MFA BRDocumento1 páginaAffiche Infection MFA BRcynthiaAinda não há avaliações
- Pharyngitis-Soothing The ThroatDocumento8 páginasPharyngitis-Soothing The ThroatridikittyAinda não há avaliações
- ArticulosDocumento5 páginasArticulosGrecia Alí AceroAinda não há avaliações
- Microbiology and Management of Peritonsillar, Retropharyngeal, and Parapharyngeal AbscessesDocumento6 páginasMicrobiology and Management of Peritonsillar, Retropharyngeal, and Parapharyngeal AbscessesVenter CiprianAinda não há avaliações
- Sars-Cov-2 Variants and Vaccines: Special ReportDocumento8 páginasSars-Cov-2 Variants and Vaccines: Special ReportRosamel FierroAinda não há avaliações
- ARDS Nuevas TerapiasDocumento3 páginasARDS Nuevas TerapiasEvelyn CóndorAinda não há avaliações
- Medical History Record FormDocumento4 páginasMedical History Record FormDaria BarannikAinda não há avaliações
- Surveilence Hais: Dr. Elsye Maria Rosa, M.KepDocumento9 páginasSurveilence Hais: Dr. Elsye Maria Rosa, M.KepEni MuchlisohAinda não há avaliações
- Biomérieux: Environmental Infection Control in HospitalsDocumento25 páginasBiomérieux: Environmental Infection Control in HospitalsYohana Fransisca WapiniAinda não há avaliações
- E-Poster Enterics For Global Health Shigella Surveillance StudyDocumento1 páginaE-Poster Enterics For Global Health Shigella Surveillance StudyNeyama AlladinAinda não há avaliações
- Optimization of Nursing Management Round 5ad3bdbbDocumento11 páginasOptimization of Nursing Management Round 5ad3bdbbsarvitaAinda não há avaliações
- The Effect of Turbinate Injection of Botulinum Toxin A On The Symptoms of Idiopathic RhinitisDocumento8 páginasThe Effect of Turbinate Injection of Botulinum Toxin A On The Symptoms of Idiopathic Rhinitismelon segerAinda não há avaliações
- Faringitis Fadhilla Annisa Efendi-1840312436Documento15 páginasFaringitis Fadhilla Annisa Efendi-1840312436fadhilla annisa efendiAinda não há avaliações
- Art 09Documento6 páginasArt 09Wiltor Kenner Rojas VillanuevaAinda não há avaliações
- Nhs Bronchiolitis Pathway Acute Setting South East Coast SCNDocumento2 páginasNhs Bronchiolitis Pathway Acute Setting South East Coast SCNdrgrizahAinda não há avaliações
- International Journal of Infectious DiseasesDocumento31 páginasInternational Journal of Infectious DiseasesAnonymous VXZymiAinda não há avaliações
- Vaccinegate:: Final Technical Report Molecular Profile Analysis of VaccineDocumento4 páginasVaccinegate:: Final Technical Report Molecular Profile Analysis of VaccineYiota KokkorisAinda não há avaliações
- Diarrhoea-Vomiting Pathway-Primary Care MAY 2015Documento2 páginasDiarrhoea-Vomiting Pathway-Primary Care MAY 2015nimraAinda não há avaliações
- Gastroenteritis PPT BonghanoyDocumento7 páginasGastroenteritis PPT BonghanoyELAINE ESTRERAAinda não há avaliações
- Cross Species Transmission of The Newly Identified Coronavirus 2019 nCoV - Ji - 2020 - Journal of MeDocumento1 páginaCross Species Transmission of The Newly Identified Coronavirus 2019 nCoV - Ji - 2020 - Journal of Metd5xb7w4dpAinda não há avaliações
- COVID-19 VACCINES THE 501Y.V2 Variant MLO HEALTH EDITDocumento3 páginasCOVID-19 VACCINES THE 501Y.V2 Variant MLO HEALTH EDITMelissa Albertyn-BrowneAinda não há avaliações
- Drug StudyDocumento16 páginasDrug StudygabbyAinda não há avaliações
- Objectives: Table 1. Selected Etiologies of Sore ThroatDocumento12 páginasObjectives: Table 1. Selected Etiologies of Sore ThroatRANIAinda não há avaliações
- Procalcitonin: BiomérieuxDocumento25 páginasProcalcitonin: Biomérieuxshafwan suyutiAinda não há avaliações
- SETTLING THE VIRUS DEBATE SourceDocumento2 páginasSETTLING THE VIRUS DEBATE SourceNina VictorAinda não há avaliações
- Acute TonsillopharyngitisDocumento9 páginasAcute TonsillopharyngitisMohammed HarisAinda não há avaliações
- Poster Caitlin BrennanDocumento1 páginaPoster Caitlin Brennansagun maharjanAinda não há avaliações
- Vacunas y Varantes Sars-Cov 2 Nejm 25-3-2021Documento3 páginasVacunas y Varantes Sars-Cov 2 Nejm 25-3-2021Cristhian Hormazabal WagnerAinda não há avaliações
- Period Dont Stop For PandemicDocumento1 páginaPeriod Dont Stop For PandemicMaria Nativity BanarioAinda não há avaliações
- White Paper Experimental Vaccines Covid-19 Feb 23Documento35 páginasWhite Paper Experimental Vaccines Covid-19 Feb 23Warren JamesAinda não há avaliações
- VaccinationDocumento6 páginasVaccinationJamil SalahAinda não há avaliações
- Microbiology Questions 2Documento6 páginasMicrobiology Questions 2JENNIFER JOHN MBBS2020Ainda não há avaliações
- Joy Benemor - T4-Sc-830-Aqa-Trilogy-Unit-43-Infection-And-Response-Foundation-Revision-Activity-Mat-Pack-English - Ver - 1Documento4 páginasJoy Benemor - T4-Sc-830-Aqa-Trilogy-Unit-43-Infection-And-Response-Foundation-Revision-Activity-Mat-Pack-English - Ver - 1v2jj5qfhjpAinda não há avaliações
- Can Trichomoniasis Cause Pharyngitis? A Case Report: Kitty Carter-Wicker, Onameyore Utuama and Folashade OmoleDocumento3 páginasCan Trichomoniasis Cause Pharyngitis? A Case Report: Kitty Carter-Wicker, Onameyore Utuama and Folashade OmoleradenbagasAinda não há avaliações
- Pemphigus VulgarisDocumento2 páginasPemphigus Vulgariszendah123Ainda não há avaliações
- To Test Your E/m Coding SkillsDocumento7 páginasTo Test Your E/m Coding SkillsLuke Rachel WurzAinda não há avaliações
- Nursing Sheet3Documento2 páginasNursing Sheet3Luke Rachel WurzAinda não há avaliações
- 01-08-2012 07 49 21PMDocumento1 página01-08-2012 07 49 21PMLuke Rachel WurzAinda não há avaliações
- Chapter 38 NS1030 Sue Study GuideDocumento19 páginasChapter 38 NS1030 Sue Study GuideLuke Rachel WurzAinda não há avaliações
- WatsuDocumento5 páginasWatsuTIME-TREVELER100% (1)
- SEO Roadmap - Bayut & DubizzleDocumento17 páginasSEO Roadmap - Bayut & Dubizzlebasel kotbAinda não há avaliações
- Afghanistan Law Bibliography 3rd EdDocumento28 páginasAfghanistan Law Bibliography 3rd EdTim MathewsAinda não há avaliações
- Case Study On TQMDocumento20 páginasCase Study On TQMshinyshani850% (1)
- Software Development Life CycleDocumento70 páginasSoftware Development Life CycleChaitanya MalikAinda não há avaliações
- MU151 Group Assignment 6Documento3 páginasMU151 Group Assignment 6Jay CadienteAinda não há avaliações
- AC2104 - Seminar 5Documento3 páginasAC2104 - Seminar 5Rachel LiuAinda não há avaliações
- Modbus Manual TD80 PDFDocumento34 páginasModbus Manual TD80 PDFAmar ChavanAinda não há avaliações
- EP105Use of English ArantxaReynosoDocumento6 páginasEP105Use of English ArantxaReynosoArantxaSteffiAinda não há avaliações
- Functions of Ecgc and Exim BankDocumento12 páginasFunctions of Ecgc and Exim BankbhumishahAinda não há avaliações
- Role LibrariesDocumento57 páginasRole LibrariesGiovanni AnggastaAinda não há avaliações
- Gaulish DictionaryDocumento4 páginasGaulish DictionarywoodwyseAinda não há avaliações
- Virtual Verde Release Plan Emails: Email 1Documento4 páginasVirtual Verde Release Plan Emails: Email 1Violet StarAinda não há avaliações
- Chemistry Important Questions-2015-2016Documento19 páginasChemistry Important Questions-2015-2016janu50% (4)
- A Guide To FractionsDocumento18 páginasA Guide To FractionsAnnelyanne RufinoAinda não há avaliações
- UntitledDocumento8 páginasUntitledMara GanalAinda não há avaliações
- Sample ProposalDocumento2 páginasSample ProposaltoupieAinda não há avaliações
- Read Chapter 4 Minicase: Fondren Publishing, Inc. From The Sales Force Management Textbook by Mark W. Johnston & Greg W. MarshallDocumento1 páginaRead Chapter 4 Minicase: Fondren Publishing, Inc. From The Sales Force Management Textbook by Mark W. Johnston & Greg W. MarshallKJRAinda não há avaliações
- Pengaruh Kompetensi Spiritual Guru Pendidikan Agama Kristen Terhadap Pertumbuhan Iman SiswaDocumento13 páginasPengaruh Kompetensi Spiritual Guru Pendidikan Agama Kristen Terhadap Pertumbuhan Iman SiswaK'lala GrianAinda não há avaliações
- Performance Task in Mathematics 10 First Quarter: GuidelinesDocumento2 páginasPerformance Task in Mathematics 10 First Quarter: Guidelinesbelle cutiee100% (3)
- What Does The Scripture Say - ' - Studies in The Function of Scripture in Early Judaism and Christianity, Volume 1 - The Synoptic GospelsDocumento149 páginasWhat Does The Scripture Say - ' - Studies in The Function of Scripture in Early Judaism and Christianity, Volume 1 - The Synoptic GospelsCometa Halley100% (1)
- English 7 Compare Contrast The People Could Fly Harriet TubmanDocumento3 páginasEnglish 7 Compare Contrast The People Could Fly Harriet Tubmanapi-508729334Ainda não há avaliações
- Native Americans - Clothing & Head DressesDocumento28 páginasNative Americans - Clothing & Head DressesThe 18th Century Material Culture Resource Center100% (15)
- SKI Report2008 - 50 2Documento46 páginasSKI Report2008 - 50 2nada safitriAinda não há avaliações
- Practical Interpretation and Application of Exoc Rine Panc Rea Tic Tes Ting in Small AnimalsDocumento20 páginasPractical Interpretation and Application of Exoc Rine Panc Rea Tic Tes Ting in Small Animalsl.fernandagonzalez97Ainda não há avaliações
- Gian Lorenzo BerniniDocumento12 páginasGian Lorenzo BerniniGiulia Galli LavigneAinda não há avaliações
- IPA Digital Media Owners Survey Autumn 2010Documento33 páginasIPA Digital Media Owners Survey Autumn 2010PaidContentUKAinda não há avaliações
- Complexity. Written Language Is Relatively More Complex Than Spoken Language. ..Documento3 páginasComplexity. Written Language Is Relatively More Complex Than Spoken Language. ..Toddler Channel TVAinda não há avaliações
- Bignay Chap 1 3 2Documento22 páginasBignay Chap 1 3 2Ralph AJ BalmesAinda não há avaliações
- Introduction To Professional School Counseling Advocacy Leadership and Intervention Ebook PDF VersionDocumento62 páginasIntroduction To Professional School Counseling Advocacy Leadership and Intervention Ebook PDF Versionmary.krueger918100% (50)