Você também pode gostar
- Limits of Effective Cough-Augmentation Techniques in Patients With Neuromuscular DiseaseDocumento8 páginasLimits of Effective Cough-Augmentation Techniques in Patients With Neuromuscular DiseasedanielAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Medi Adores Dis Fun CM LDocumento7 páginasMedi Adores Dis Fun CM LdanielAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Physiotherapy and Weaning From Prolonged Mechanical VentilationDocumento9 páginasPhysiotherapy and Weaning From Prolonged Mechanical VentilationdanielAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Asthma-Specific Health Related Quality of Life of People in Great Britain: A National SurveyDocumento42 páginasAsthma-Specific Health Related Quality of Life of People in Great Britain: A National SurveydanielAinda não há avaliações
- Vol Pulmon Art AcDocumento7 páginasVol Pulmon Art AcdanielAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Pulmonary Pharmacology & TherapeuticsDocumento13 páginasPulmonary Pharmacology & TherapeuticsdanielAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- AVDenBrasilerasAsmaticas PDFDocumento7 páginasAVDenBrasilerasAsmaticas PDFdanielAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Asthma in The Older Adult: Presentation, Considerations and Clinical ManagementDocumento13 páginasAsthma in The Older Adult: Presentation, Considerations and Clinical ManagementdanielAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Exercise Deactivates Leukocytes in Asthma: AuthorsDocumento9 páginasExercise Deactivates Leukocytes in Asthma: AuthorsdanielAinda não há avaliações
- Association Between Maximal Aerobic Capacity and Psychosocial Factors in Adults With Moderate-to-Severe AsthmaDocumento5 páginasAssociation Between Maximal Aerobic Capacity and Psychosocial Factors in Adults With Moderate-to-Severe AsthmadanielAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Asthma and Aerobic Exercise: A Review of The Empirical LiteratureDocumento23 páginasAsthma and Aerobic Exercise: A Review of The Empirical LiteraturedanielAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Continuous Positive Airway Pressure Cpap in Neonatal UnitsDocumento2 páginasContinuous Positive Airway Pressure Cpap in Neonatal Unitsnadhifa akAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- NCP For Ineffective Breathing Pattern - RMC CasepressDocumento2 páginasNCP For Ineffective Breathing Pattern - RMC Casepressmissyuri08Ainda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Chester Step Test en EPOCDocumento9 páginasChester Step Test en EPOChuevazooo04Ainda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- PFT Final Exam Study Guide & Practice QuestionsDocumento38 páginasPFT Final Exam Study Guide & Practice QuestionsJade Louise FkshmAinda não há avaliações
- NIV (Non-Invasive Ventilation) : Dr.S.MagimaiguberanDocumento38 páginasNIV (Non-Invasive Ventilation) : Dr.S.MagimaiguberanDr mahi sAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- 1.e. Bronchiolitis Treatment & Management - Approach Considerations, Initial Management, Admission CriteriaDocumento12 páginas1.e. Bronchiolitis Treatment & Management - Approach Considerations, Initial Management, Admission CriteriaDavid CraigAinda não há avaliações
- Draft July 15 - 16 Participant ListDocumento107 páginasDraft July 15 - 16 Participant Listashakow8849Ainda não há avaliações
- CPAPDocumento11 páginasCPAPpreeti19987100% (1)
- B2 - A - Cystic FibrosisDocumento1 páginaB2 - A - Cystic FibrosisfaisalAinda não há avaliações
- PhysioEx Exercise 7 ActivityDocumento3 páginasPhysioEx Exercise 7 ActivityCLAUDIA ELISABET BECERRA GONZALESAinda não há avaliações
- Asthma and Other Respiratory Medications DefindDocumento4 páginasAsthma and Other Respiratory Medications DefindKiran ManojAinda não há avaliações
- Effectiveness of Nebulised Salbutamol Administered in Ambulances To Patients With Severe Acute AsthmaDocumento4 páginasEffectiveness of Nebulised Salbutamol Administered in Ambulances To Patients With Severe Acute AsthmaMaria ClaraAinda não há avaliações
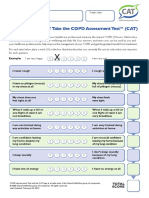
- How Is Your Copd? Take The Copd Assessmenttest (Cat) : Your Name: Today'S DateDocumento1 páginaHow Is Your Copd? Take The Copd Assessmenttest (Cat) : Your Name: Today'S DateAndreea BurceaAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Postural DrainageDocumento13 páginasPostural DrainageMelisande Rae CiruelaAinda não há avaliações
- Exploring The Innovation in Pulmonary and Respiratory MedicineDocumento2 páginasExploring The Innovation in Pulmonary and Respiratory MedicineJamalAinda não há avaliações
- ICU Physiology in 1000 Words: Driving Pressure & Stress IndexDocumento5 páginasICU Physiology in 1000 Words: Driving Pressure & Stress Indexaniket mittalAinda não há avaliações
- BOOK Spirometry in PracticeDocumento104 páginasBOOK Spirometry in Practicenadeem khan100% (1)
- Format Askep GadarDocumento6 páginasFormat Askep GadarveraarizkiAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Bronchiectasis: Yuping GuoDocumento75 páginasBronchiectasis: Yuping GuoAmeliaAinda não há avaliações
- Neuro Sample QuestionsDocumento14 páginasNeuro Sample Questionsanonymousah777Ainda não há avaliações
- Check List of Oxygen Administration For LevelDocumento4 páginasCheck List of Oxygen Administration For LevelFikir Ligisinaw AyalkimAinda não há avaliações
- Obat Yang Bekerja Pada Saluran NapasDocumento21 páginasObat Yang Bekerja Pada Saluran NapaszaroziAinda não há avaliações
- Kronik. Fakultas Kedokteran Universitas Lampung. J Majority: Vol 4 No 5Documento2 páginasKronik. Fakultas Kedokteran Universitas Lampung. J Majority: Vol 4 No 5ayu praptiAinda não há avaliações
- Mount Sinai ICUDocumento642 páginasMount Sinai ICUMahmoud FathyAinda não há avaliações
- Addressing Current Management of Asthma in children-FKUIDocumento28 páginasAddressing Current Management of Asthma in children-FKUICane MochiAinda não há avaliações
- Pulmonary Function TestDocumento7 páginasPulmonary Function TestGhada HusseinAinda não há avaliações
- BronchiectasisDocumento61 páginasBronchiectasisRapid MedicineAinda não há avaliações
- Arya - Usefulness and Safety of Transbronchial Biopsy With Large Forceps During Flexible BronchosDocumento5 páginasArya - Usefulness and Safety of Transbronchial Biopsy With Large Forceps During Flexible BronchosXaralyn XaviereAinda não há avaliações
- Management of ARDS in AdultsDocumento2 páginasManagement of ARDS in AdultsCarlos PalominoAinda não há avaliações
- Spesifikasi - VYGON Emergency APO CPAP KitDocumento2 páginasSpesifikasi - VYGON Emergency APO CPAP KitNanno LadowogoAinda não há avaliações