Você também pode gostar
- Malignant Bone TumoursDocumento67 páginasMalignant Bone Tumoursmie_anumAinda não há avaliações
- Hyperthyroidism and Thyroid Storm: Causes, Symptoms, and TreatmentDocumento44 páginasHyperthyroidism and Thyroid Storm: Causes, Symptoms, and TreatmentCharith KumaraAinda não há avaliações
- Menorrhagia Seminar 7Documento26 páginasMenorrhagia Seminar 7mie_anumAinda não há avaliações
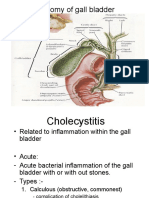
- Acute Cholecystitis Cp2 Surgery by HelmyDocumento17 páginasAcute Cholecystitis Cp2 Surgery by Helmymie_anumAinda não há avaliações
- CP Primary Care AntenatalDocumento37 páginasCP Primary Care Antenatalmie_anumAinda não há avaliações
- Postpartum Hemorrhage Due To Uterine AtonyDocumento30 páginasPostpartum Hemorrhage Due To Uterine Atonymie_anum88% (8)
- Case Write-Up: OphthalmologyDocumento9 páginasCase Write-Up: Ophthalmologymie_anumAinda não há avaliações
- Mohd Helmy B Abu Bakar Farrah Hanna BT Mohd Nasir Khairunisa BT JuhariDocumento24 páginasMohd Helmy B Abu Bakar Farrah Hanna BT Mohd Nasir Khairunisa BT Juharimie_anumAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- AntepartumDocumento32 páginasAntepartumphoenix180100% (1)
- Kapampangan Cultural FactorsDocumento5 páginasKapampangan Cultural FactorsTroy MagcalasAinda não há avaliações
- Reproduction in Lower and Higher AnimalsDocumento2 páginasReproduction in Lower and Higher Animalssamarpeetnandanwar21Ainda não há avaliações
- Women's Right to Choose AbortionDocumento10 páginasWomen's Right to Choose AbortionRamizAinda não há avaliações
- Anatomy and Physiology Chapter OverviewDocumento6 páginasAnatomy and Physiology Chapter OverviewJun ManAinda não há avaliações
- Beeja SphutaDocumento5 páginasBeeja SphutaS K MishraAinda não há avaliações
- Am I A Juvenile DelinquentDocumento3 páginasAm I A Juvenile DelinquentJiffy MaghanoyAinda não há avaliações
- Cancer of Reproductive SystemDocumento42 páginasCancer of Reproductive SystemPia SempronAinda não há avaliações
- Theriogenology: S. Fierro, C. Vi Noles, J. Olivera-MuzanteDocumento5 páginasTheriogenology: S. Fierro, C. Vi Noles, J. Olivera-MuzanteViviana CarrilloAinda não há avaliações
- Biología Del Cuerpo LuteoDocumento12 páginasBiología Del Cuerpo LuteoVioleta v cAinda não há avaliações
- How To Dissect A SharkDocumento14 páginasHow To Dissect A SharkgregAinda não há avaliações
- The Endocrine SystemDocumento12 páginasThe Endocrine Systemmagma_pt9888Ainda não há avaliações
- Ethics Module 4Documento4 páginasEthics Module 4Joseph TheThirdAinda não há avaliações
- Pedigree QuestionsDocumento4 páginasPedigree QuestionsSaumya SelvarajiAinda não há avaliações
- Genital HerpesDocumento2 páginasGenital HerpesWisnu WardanaAinda não há avaliações
- Ian DonaldDocumento13 páginasIan DonaldBalasan Cristina-GabrielaAinda não há avaliações
- Running Head: Teen Birth Disparities in Sarasota 1Documento15 páginasRunning Head: Teen Birth Disparities in Sarasota 1api-456052042Ainda não há avaliações
- Tittle: Human As A Complex OrganismDocumento21 páginasTittle: Human As A Complex OrganismNick LeeAinda não há avaliações
- Abscess Scrotum DrainageDocumento7 páginasAbscess Scrotum DrainageRosyAinda não há avaliações
- Aipmtts15t06 SolutionDocumento50 páginasAipmtts15t06 SolutionSouradeep DebAinda não há avaliações
- Micromanipulation techniquesDocumento6 páginasMicromanipulation techniquesSai SridharAinda não há avaliações
- Evidence Based Practice Approach)Documento13 páginasEvidence Based Practice Approach)Yopie AdlieAinda não há avaliações
- Normal LabourDocumento185 páginasNormal LabourAnnapurna Dangeti100% (1)
- Tugas Mata Kuliah Bahasa Inggris: Dosen Pembimbing: A. M. Aziz, M. PDDocumento4 páginasTugas Mata Kuliah Bahasa Inggris: Dosen Pembimbing: A. M. Aziz, M. PDMega Safira MahardiniAinda não há avaliações
- Reproductive System FunctionsDocumento3 páginasReproductive System FunctionsVernice OrtegaAinda não há avaliações
- Admission of Term Infants To The NicuDocumento6 páginasAdmission of Term Infants To The NicucarlsonrenovatioAinda não há avaliações
- Tiburones: de México, Centro América y El CaribeDocumento2 páginasTiburones: de México, Centro América y El CaribePeGaZuS911 GaMePLaY y Animacion FlorezAinda não há avaliações
- Respiratory of GrasshopperDocumento137 páginasRespiratory of GrasshopperSadman Ishraq SayefAinda não há avaliações
- The Following Text Is For Questions 1 To 3Documento5 páginasThe Following Text Is For Questions 1 To 3Alfi HasanahAinda não há avaliações
- A Pilot Evaluation of Saline Sonohysterography For Postmenopausal Bleeding With Thickened EndometriumDocumento4 páginasA Pilot Evaluation of Saline Sonohysterography For Postmenopausal Bleeding With Thickened EndometriumAna Di JayaAinda não há avaliações