Você também pode gostar
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderNo EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderAinda não há avaliações
- Rol de La Endoscopia en La Sospecha de ColedocolitiasisDocumento9 páginasRol de La Endoscopia en La Sospecha de ColedocolitiasisGerardo Paul Santana BazalarAinda não há avaliações
- Fast Facts: Cholangiocarcinoma: Diagnostic and therapeutic advances are improving outcomesNo EverandFast Facts: Cholangiocarcinoma: Diagnostic and therapeutic advances are improving outcomesAinda não há avaliações
- Intraoperative CholangiographyDocumento6 páginasIntraoperative CholangiographyPolly LombardiniAinda não há avaliações
- The Value of MRCPDocumento5 páginasThe Value of MRCPBella YulandaAinda não há avaliações
- Renal BiopsyDocumento4 páginasRenal BiopsyDeshan AdikariAinda não há avaliações
- 1 s2.0 S0016510796700986 Main PDFDocumento8 páginas1 s2.0 S0016510796700986 Main PDFErikson SipayungAinda não há avaliações
- JR2 RizaDocumento3 páginasJR2 RizaCitra DewiAinda não há avaliações
- CNCR 23454Documento7 páginasCNCR 23454Aishwarya SinghAinda não há avaliações
- Ekjg004 03 10Documento5 páginasEkjg004 03 10HiKa SaGoAinda não há avaliações
- AACE Clinical Case Reports: John C. Parker, MD, Andreas G. Moraitis, MD, Joseph K. Belanoff, MDDocumento5 páginasAACE Clinical Case Reports: John C. Parker, MD, Andreas G. Moraitis, MD, Joseph K. Belanoff, MDMohammed Shuaib AhmedAinda não há avaliações
- 12 BuenoDocumento7 páginas12 BuenoFlipAinda não há avaliações
- Sedimento RBC DismorficCellDocumento7 páginasSedimento RBC DismorficCellecko RomanAinda não há avaliações
- Clinical Utility of MRCP in Biliary Disease.2653Documento2 páginasClinical Utility of MRCP in Biliary Disease.2653Ilham BelgaAinda não há avaliações
- Csendes1992 FR Predictores de ColangitisDocumento4 páginasCsendes1992 FR Predictores de ColangitisSebastian Sapiain GonzalezAinda não há avaliações
- Cambio de Laparoscopia A Cirugia AbiertaDocumento7 páginasCambio de Laparoscopia A Cirugia AbiertaJosé David Cortez Centeno 20190155Ainda não há avaliações
- Aresia de Vias Biliares UltrasonidoDocumento14 páginasAresia de Vias Biliares UltrasonidoArturo GarciaAinda não há avaliações
- Obstructive Jaundice Aetiological SpectrDocumento8 páginasObstructive Jaundice Aetiological Spectrvvwaghmare30Ainda não há avaliações
- Urine Sediment Exam Provides More Diagnostic Information in AKI-1Documento4 páginasUrine Sediment Exam Provides More Diagnostic Information in AKI-1Ingrid González EfronAinda não há avaliações
- Impact of Non Invasive Biomarkers On Hepatology PRDocumento17 páginasImpact of Non Invasive Biomarkers On Hepatology PRCláudia SilvaAinda não há avaliações
- Acute Transient Hepatocellular Injury in Cholelithiasis and Cholecystitis Without Evidence of CholedocholithiasisDocumento5 páginasAcute Transient Hepatocellular Injury in Cholelithiasis and Cholecystitis Without Evidence of CholedocholithiasisardytawaradaniAinda não há avaliações
- Síndrome Hepatorrenal Cirrosis Eur Gast J 2021Documento9 páginasSíndrome Hepatorrenal Cirrosis Eur Gast J 2021Anabel GonzalezAinda não há avaliações
- JurnalDocumento6 páginasJurnalAgamMayzulfiAinda não há avaliações
- Comprehensive Assessment of ECM Turnover Using Serum Biomarkers Establishes PBC As A High-Turnover Autoimmune Liver DiseaseDocumento11 páginasComprehensive Assessment of ECM Turnover Using Serum Biomarkers Establishes PBC As A High-Turnover Autoimmune Liver Diseasestefania.popescu153Ainda não há avaliações
- Flores - TVTDocumento9 páginasFlores - TVTChristian De LeonAinda não há avaliações
- Liver Transplantation Using Grafts of Living Donors With Isolated Unconjugated Hyperbilirubinemia: A Matched Case - Control StudyDocumento8 páginasLiver Transplantation Using Grafts of Living Donors With Isolated Unconjugated Hyperbilirubinemia: A Matched Case - Control StudytrisyAinda não há avaliações
- Clinical Imaging: Small-Bowel Obstruction: State-of-the-Art Imaging and Its Role in Clinical ManagementDocumento1 páginaClinical Imaging: Small-Bowel Obstruction: State-of-the-Art Imaging and Its Role in Clinical ManagementDavis KallanAinda não há avaliações
- 10.1007@s11605 018 04090 ZDocumento11 páginas10.1007@s11605 018 04090 ZGabriel RangelAinda não há avaliações
- Biomarcadores Post Aki A ErcDocumento12 páginasBiomarcadores Post Aki A ErcGiss UrizarAinda não há avaliações
- Evaluation of Specific Cytomorphologic Features and CA19-9 LevelsDocumento6 páginasEvaluation of Specific Cytomorphologic Features and CA19-9 LevelsТетяна МагасьAinda não há avaliações
- Pediatric Non-Hodgkin Lymphoma Workup - Approach Considerations, Laboratory Studies, Imaging StudiesDocumento5 páginasPediatric Non-Hodgkin Lymphoma Workup - Approach Considerations, Laboratory Studies, Imaging StudiestopAinda não há avaliações
- The Definition of Acute Kidney Injury and Its Use in PracticeDocumento12 páginasThe Definition of Acute Kidney Injury and Its Use in PracticewelinAinda não há avaliações
- Ce 46 476Documento5 páginasCe 46 476KIKIAinda não há avaliações
- 44 Year Old Man With Fatigue, Weight Loss, and LeuDocumento5 páginas44 Year Old Man With Fatigue, Weight Loss, and LeuRamiro Arraya MierAinda não há avaliações
- Bile Duct DilatedDocumento4 páginasBile Duct DilatedAmit GauravAinda não há avaliações
- Acut Kidney InjuryDocumento12 páginasAcut Kidney InjuryorriAinda não há avaliações
- Clinical Spotlight Review For The Management of CholedocholithiasisDocumento10 páginasClinical Spotlight Review For The Management of CholedocholithiasisLourdes MarquezAinda não há avaliações
- Endourology and Stones Predictive Value of Leukocytosis For Infectious Complications After Percutaneous NephrolithotomyDocumento5 páginasEndourology and Stones Predictive Value of Leukocytosis For Infectious Complications After Percutaneous NephrolithotomyJufrialdy AldyAinda não há avaliações
- Bitcoin DiscussionDocumento6 páginasBitcoin Discussionmrpoopy123Ainda não há avaliações
- Bilirrubina en Liq OrgánicoDocumento6 páginasBilirrubina en Liq OrgánicoCindy Yunuen LeónAinda não há avaliações
- Bmri2019 3951574Documento10 páginasBmri2019 3951574Anonymous 1EQutBAinda não há avaliações
- Informed Consent in Elective and Emergency LaparosDocumento2 páginasInformed Consent in Elective and Emergency LaparosFadi NasrallahAinda não há avaliações
- Changes in Urine Volume and Serum Albumin in Incident Hemodialysis PatientsDocumento12 páginasChanges in Urine Volume and Serum Albumin in Incident Hemodialysis Patientsmelda lestari haidirAinda não há avaliações
- Kidneydiseaseandthe Nexusofchronickidney DiseaseandacutekidneyinjuryDocumento33 páginasKidneydiseaseandthe Nexusofchronickidney DiseaseandacutekidneyinjuryMardauc AnaidAinda não há avaliações
- The New Age of Renal Biomarkers - Does SDMA Solve All of Our ProblemsDocumento11 páginasThe New Age of Renal Biomarkers - Does SDMA Solve All of Our ProblemsCabinet VeterinarAinda não há avaliações
- A Randomized Controlled Trial of Emergency Treatment of Bleeding Esophageal Varices in Cirrhosis For Hepatocellular CarcinomaDocumento15 páginasA Randomized Controlled Trial of Emergency Treatment of Bleeding Esophageal Varices in Cirrhosis For Hepatocellular CarcinomaAntonius SimangunsongAinda não há avaliações
- Hepatorenal SyndromeDocumento14 páginasHepatorenal SyndromeVerónica Duménez JofréAinda não há avaliações
- Low Hemoglobin Levels Are Associated With Upper Gastrointestinal BleedingDocumento4 páginasLow Hemoglobin Levels Are Associated With Upper Gastrointestinal BleedingYdha FpAinda não há avaliações
- BM 27 153Documento24 páginasBM 27 153Imam albanjariAinda não há avaliações
- Modern Imaging in Obstructive JaundiceDocumento4 páginasModern Imaging in Obstructive JaundicedanaogreanuAinda não há avaliações
- Fibroscan: Hepatitis CDocumento4 páginasFibroscan: Hepatitis CMuhammad Halil GibranAinda não há avaliações
- Accuracy of ASGE Criteria For The Prediction of Choledocholithiasis 2016Documento6 páginasAccuracy of ASGE Criteria For The Prediction of Choledocholithiasis 2016DannyAinda não há avaliações
- Differences in Nutritional Risk Assessment Between NRS2002, RFH-NPT and LDUST in Cirrhotic PatientsDocumento8 páginasDifferences in Nutritional Risk Assessment Between NRS2002, RFH-NPT and LDUST in Cirrhotic PatientsMasna ArahmanAinda não há avaliações
- Renal Biopsy of Dogs and CatsDocumento12 páginasRenal Biopsy of Dogs and CatsfrankyAinda não há avaliações
- Sampling and Reporting of Inflammatory Bowel DiseaseDocumento12 páginasSampling and Reporting of Inflammatory Bowel DiseaseDiego Fernando Ortiz TenorioAinda não há avaliações
- Ultrasound Spleen Morphology, But Not Vascular Liver Doppler MeasuresDocumento1 páginaUltrasound Spleen Morphology, But Not Vascular Liver Doppler MeasuresdenisegmeloAinda não há avaliações
- Advantages of Laparoscopic Common Bile Duct Exploration in Common Bile Duct StonesDocumento5 páginasAdvantages of Laparoscopic Common Bile Duct Exploration in Common Bile Duct Stonesnaili nsnAinda não há avaliações
- ACG Clinical Guideline: Primary Sclerosing CholangitisDocumento14 páginasACG Clinical Guideline: Primary Sclerosing Cholangitisragil putra jAinda não há avaliações
- Biomarcadores en AKIDocumento14 páginasBiomarcadores en AKIhemer hadyn calderon alvitesAinda não há avaliações
- Disorders of PancreasDocumento17 páginasDisorders of PancreasjonasAinda não há avaliações
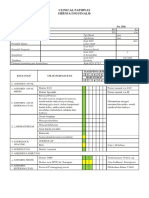
- Clinical Pathway Apendisitis AcutaDocumento7 páginasClinical Pathway Apendisitis AcutaTina HerreraAinda não há avaliações
- Jurnal PoneDocumento21 páginasJurnal PoneTina HerreraAinda não há avaliações
- CP HerniaDocumento6 páginasCP HerniaTina HerreraAinda não há avaliações
- Clinical Pathway Limphadenopaty ColiDocumento6 páginasClinical Pathway Limphadenopaty ColiTina HerreraAinda não há avaliações
- Tumor Immune Escape Mechanisms: Yi Ting Koh,, M. Luz García-Hernández,, and W. Martin KastDocumento26 páginasTumor Immune Escape Mechanisms: Yi Ting Koh,, M. Luz García-Hernández,, and W. Martin KastTina HerreraAinda não há avaliações
- Wjps 7 016 PDFDocumento9 páginasWjps 7 016 PDFTina HerreraAinda não há avaliações
- Thoracic Lumbar, Eko AgusDocumento32 páginasThoracic Lumbar, Eko AgusTina HerreraAinda não há avaliações
- Intracranial Pathophysiology, Zainal MDocumento25 páginasIntracranial Pathophysiology, Zainal MTina HerreraAinda não há avaliações
- Brain Protection, M.Ramli PDFDocumento50 páginasBrain Protection, M.Ramli PDFTina HerreraAinda não há avaliações
- Brain Protection, M.Ramli PDFDocumento50 páginasBrain Protection, M.Ramli PDFTina HerreraAinda não há avaliações
- Soal Ujian Neurotrauma Full - JWBDocumento22 páginasSoal Ujian Neurotrauma Full - JWBTina HerreraAinda não há avaliações
- 09.daftar Pustaka FixDocumento4 páginas09.daftar Pustaka FixTina HerreraAinda não há avaliações
- Biomelecular Aspect, Irawan YusufDocumento23 páginasBiomelecular Aspect, Irawan YusufTina HerreraAinda não há avaliações
- Teks Lagu NatalDocumento4 páginasTeks Lagu NatalTina HerreraAinda não há avaliações
- Template EnglishDocumento15 páginasTemplate EnglishTina HerreraAinda não há avaliações
- Kurnia Ari / 23 THN / MR: 16020635 Admission: 01-02-2016 Consultant: Dr. Almahitta, Spbp-ReDocumento7 páginasKurnia Ari / 23 THN / MR: 16020635 Admission: 01-02-2016 Consultant: Dr. Almahitta, Spbp-ReTina HerreraAinda não há avaliações
- Althea NCM 116aDocumento192 páginasAlthea NCM 116aspain michaelisAinda não há avaliações
- Dispensary Investigation Details - Ramakrishna Math (Yogodyan)Documento9 páginasDispensary Investigation Details - Ramakrishna Math (Yogodyan)HIMANSHU KUMAR CHOUDHARYAinda não há avaliações
- YNM Part 2 - ExplainDocumento61 páginasYNM Part 2 - ExplainCHAKRADHARA RAO100% (1)
- Clinical Chemistry 2 TransDocumento36 páginasClinical Chemistry 2 TransAlyssa Taylor LopezAinda não há avaliações
- Cheetsheet 6Documento1 páginaCheetsheet 6Rick Frea92% (12)
- LIVERHEALTH2022Documento103 páginasLIVERHEALTH2022Krisztina Borkóné FodorAinda não há avaliações
- GIT Cirrhosis Liver in ChildrenDocumento37 páginasGIT Cirrhosis Liver in ChildrenDr.P.NatarajanAinda não há avaliações
- Ramadanandliverdisorders PDFDocumento7 páginasRamadanandliverdisorders PDFRaissa Virgy RiandaAinda não há avaliações
- Non Viral HepatitisDocumento40 páginasNon Viral Hepatitisostaz2000100% (1)
- Gastroenterology Case Discussion: JANUARY 07, 2021 Dr. Stephen Wong Indigo and VioletDocumento19 páginasGastroenterology Case Discussion: JANUARY 07, 2021 Dr. Stephen Wong Indigo and VioletJolaine ValloAinda não há avaliações
- Efficacy of Ursodeoxycholic Acid in Nonalcoholic Fatty Liver Disease: An Updated Meta-Analysis of Randomized Controlled TrialsDocumento10 páginasEfficacy of Ursodeoxycholic Acid in Nonalcoholic Fatty Liver Disease: An Updated Meta-Analysis of Randomized Controlled Trialssteventanco1977Ainda não há avaliações
- Catalog (ENG) May Sinh Hoa Tu Dong BS-600Documento4 páginasCatalog (ENG) May Sinh Hoa Tu Dong BS-600anhhp8xAinda não há avaliações
- Wilson DiseaseDocumento16 páginasWilson DiseaseFranco Fabricio CarpioAinda não há avaliações
- RX DaytonaDocumento16 páginasRX Daytonajedi_exAinda não há avaliações
- HELLP Syndrome (Hemolysis, Elevated Liver Enzymes, and Low Platelets) - UpToDateDocumento44 páginasHELLP Syndrome (Hemolysis, Elevated Liver Enzymes, and Low Platelets) - UpToDateMaribel Romero GalíndezAinda não há avaliações
- Liver EnzymesDocumento6 páginasLiver EnzymesWande AyodeleAinda não há avaliações
- Careplan Medication by ProxyDocumento21 páginasCareplan Medication by Proxytitah_294Ainda não há avaliações
- Clinical Study On The Efficacy of Eranda Beeja Anjana in The Management of KamalaDocumento3 páginasClinical Study On The Efficacy of Eranda Beeja Anjana in The Management of KamalaEditor IJTSRDAinda não há avaliações
- Basic Pharmacology For Nurses 15th Edition Clayton Test BankDocumento10 páginasBasic Pharmacology For Nurses 15th Edition Clayton Test Bankclaraninht5sqdj100% (37)
- DR Jockers Cleanse Your Liver Now UpdatedDocumento102 páginasDR Jockers Cleanse Your Liver Now UpdatedfizzAinda não há avaliações
- Gastrointestinal System (Letu Da) PDFDocumento74 páginasGastrointestinal System (Letu Da) PDFNafiul Islam100% (4)
- V2 - STD - Barang - Farmasi 20021Documento36 páginasV2 - STD - Barang - Farmasi 20021anthonyAinda não há avaliações
- Acasestudyoncirrhosisofliver 160424143748Documento48 páginasAcasestudyoncirrhosisofliver 160424143748michelleAinda não há avaliações
- Multi Sera Calibrator: Value Sheet of Mindray BS Measurement SystemDocumento4 páginasMulti Sera Calibrator: Value Sheet of Mindray BS Measurement SystemAngel50% (2)
- RFP - Provision of Medical ServicesDocumento10 páginasRFP - Provision of Medical ServicesABC tradingAinda não há avaliações
- GNRC Health PackageDocumento4 páginasGNRC Health PackageAakashSamaddarAinda não há avaliações
- Icteric Index and Its SignificanceDocumento3 páginasIcteric Index and Its SignificanceJulius FrondaAinda não há avaliações
- Metabolism - Nursing Test QuestionsDocumento68 páginasMetabolism - Nursing Test QuestionsRNStudent1100% (2)
- Effect Centella Anti TB Drugs Vol3 - Issue5 - 02Documento6 páginasEffect Centella Anti TB Drugs Vol3 - Issue5 - 02Kiky HaryantariAinda não há avaliações
- AlcoholismDocumento24 páginasAlcoholismJay J.Ainda não há avaliações
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Nota: 3 de 5 estrelas3/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNo EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNota: 5 de 5 estrelas5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (29)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsAinda não há avaliações
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 5 de 5 estrelas5/5 (81)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNota: 2 de 5 estrelas2/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNo EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNota: 4.5 de 5 estrelas4.5/5 (328)
- The Obesity Code: Unlocking the Secrets of Weight LossNo EverandThe Obesity Code: Unlocking the Secrets of Weight LossNota: 4 de 5 estrelas4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNo EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNota: 4.5 de 5 estrelas4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNo EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNota: 4.5 de 5 estrelas4.5/5 (42)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 4 de 5 estrelas4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNota: 5 de 5 estrelas5/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNo EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNota: 4.5 de 5 estrelas4.5/5 (253)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.No EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Nota: 4.5 de 5 estrelas4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityNo EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityNota: 4 de 5 estrelas4/5 (5)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisNo EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisNota: 4 de 5 estrelas4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryNo EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryNota: 4 de 5 estrelas4/5 (45)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNo EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNota: 4.5 de 5 estrelas4.5/5 (170)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedNota: 4 de 5 estrelas4/5 (61)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesNo EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesNota: 4.5 de 5 estrelas4.5/5 (1412)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingNo EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingNota: 1 de 5 estrelas1/5 (1)
- The Marshmallow Test: Mastering Self-ControlNo EverandThe Marshmallow Test: Mastering Self-ControlNota: 4.5 de 5 estrelas4.5/5 (59)