Você também pode gostar
- UrologyDocumento12 páginasUrologyThakoon Tts100% (1)
- Clinical Examination and Applied Medicine, Volume I-Gastroenterology Series (Mar 7, 2018) - (1946646938) - (CRC Press)Documento176 páginasClinical Examination and Applied Medicine, Volume I-Gastroenterology Series (Mar 7, 2018) - (1946646938) - (CRC Press)taher100% (1)
- Autoimmune Syndromes and Inflammatory Sy PDFDocumento105 páginasAutoimmune Syndromes and Inflammatory Sy PDFdragosAinda não há avaliações
- Polygenic and Multifactorial Diseases: - Key Features and Isolation of Responsible Genes Newcastle 13th December 2007Documento34 páginasPolygenic and Multifactorial Diseases: - Key Features and Isolation of Responsible Genes Newcastle 13th December 2007Fidia FibrianaAinda não há avaliações
- Benign Prostatic Hyperplasia: Philippine Urological Association, IncDocumento7 páginasBenign Prostatic Hyperplasia: Philippine Urological Association, Incsam_llamzon100% (1)
- NBME 16 Complete PDFDocumento112 páginasNBME 16 Complete PDFSilar Khan67% (18)
- Benign Prostatic Hyperplasia Concept MapDocumento1 páginaBenign Prostatic Hyperplasia Concept MapSarah RonquilloAinda não há avaliações
- Cervical Ca CaseDocumento9 páginasCervical Ca CaseAbdullah FauziAinda não há avaliações
- Placental AbnormalitiesDocumento3 páginasPlacental AbnormalitiesThakoon TtsAinda não há avaliações
- Don Juans, Monks, and Multi-Orgasmic WormsDocumento1 páginaDon Juans, Monks, and Multi-Orgasmic WormskukutxiAinda não há avaliações
- British Biology Olympiad 2021Documento66 páginasBritish Biology Olympiad 2021Yinyin ZhuAinda não há avaliações
- CTEVDocumento17 páginasCTEVamal.fathullah100% (1)
- Wade Davis-The Ethnosphere and The Academy PDFDocumento17 páginasWade Davis-The Ethnosphere and The Academy PDFTracy Leigh HenryAinda não há avaliações
- Philippine Urological Association, Inc.: Executive Committee and Board Members 1997Documento12 páginasPhilippine Urological Association, Inc.: Executive Committee and Board Members 1997mits98Ainda não há avaliações
- Autoimmune Bullous Dermatoses - Overview of Serological Diagnostics in Blister Forming Diseases of The SkinDocumento8 páginasAutoimmune Bullous Dermatoses - Overview of Serological Diagnostics in Blister Forming Diseases of The SkinFedoxyzAinda não há avaliações
- Benign Prostate Hyperplasia: Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera UtaraDocumento56 páginasBenign Prostate Hyperplasia: Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera UtaraJessica PurbaAinda não há avaliações
- Bone HealingDocumento2 páginasBone HealingGerardLum100% (2)
- Eng ชุดที่3 4Documento26 páginasEng ชุดที่3 4Thakoon TtsAinda não há avaliações
- Benign Prostate Hyperplasia (BPH)Documento81 páginasBenign Prostate Hyperplasia (BPH)Salaxar Senpai100% (1)
- Benign Prostatic HyperthropyDocumento54 páginasBenign Prostatic HyperthropyPrawira Buntara PutraAinda não há avaliações
- P2 Breast Pathology (Patho Surg) PDFDocumento120 páginasP2 Breast Pathology (Patho Surg) PDFThakoon TtsAinda não há avaliações
- PSA Testing For Prostate Cancer Information For Well MenDocumento2 páginasPSA Testing For Prostate Cancer Information For Well MenkernowsebAinda não há avaliações
- Hematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesNo EverandHematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesNota: 5 de 5 estrelas5/5 (2)
- Benign Prostatic HyperplasiaDocumento5 páginasBenign Prostatic HyperplasiaLag Lag AlbercaAinda não há avaliações
- Medical Management of bph1Documento48 páginasMedical Management of bph1Julfikar KhanAinda não há avaliações
- Benign Prostatic HyperplasiaDocumento5 páginasBenign Prostatic Hyperplasiatabangin_hilario100% (1)
- Benign Prostatic Hyperplasia BPH: PathologyDocumento9 páginasBenign Prostatic Hyperplasia BPH: Pathologyhussain Altaher0% (1)
- GUS2 - K5 - BPH Final 1Documento52 páginasGUS2 - K5 - BPH Final 1Arifin MuhammadAinda não há avaliações
- Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera UtaraDocumento54 páginasDiv. of Urology, Dept. Surgery Medical Faculty, University of Sumatera UtaraMuhammad Mahadi HasibuanAinda não há avaliações
- Benign Prostate Hyperplasia:: Pathophysiology, Diagnosis & TreatmentDocumento52 páginasBenign Prostate Hyperplasia:: Pathophysiology, Diagnosis & TreatmentVanny SaimimaAinda não há avaliações
- Benign Prostatic HyperplasiaDocumento20 páginasBenign Prostatic HyperplasiaMohammed AadeelAinda não há avaliações
- BPH Mohit Singhania InternDocumento29 páginasBPH Mohit Singhania InternMohitAinda não há avaliações
- Benign Prostatic Hyperplasia. NCM 109Documento16 páginasBenign Prostatic Hyperplasia. NCM 109Niña Jean Tormis AldabaAinda não há avaliações
- BRT Surgery - Urology Part 2Documento3 páginasBRT Surgery - Urology Part 2Princess Sittie Asiah AbdullahAinda não há avaliações
- Fluid and ElectrolytesDocumento21 páginasFluid and ElectrolytesKc Cabanilla LizardoAinda não há avaliações
- Lecture 15-16. BPH, Stricture Urethra, Varicocele, Spermatocele, Neonatal HidronefrosisDocumento64 páginasLecture 15-16. BPH, Stricture Urethra, Varicocele, Spermatocele, Neonatal HidronefrosiskrisnadewirahadiAinda não há avaliações
- Benign Prostate Hyperplasia: Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera UtaraDocumento49 páginasBenign Prostate Hyperplasia: Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera UtaramahadianismailnstAinda não há avaliações
- Hamed Alabad BPHDocumento47 páginasHamed Alabad BPHHamed AlabadAinda não há avaliações
- Benign prostatic hyperplasia يوازمحلا يلع دمحا.د: Epidemiology of BPHDocumento8 páginasBenign prostatic hyperplasia يوازمحلا يلع دمحا.د: Epidemiology of BPHAli SafaaAinda não há avaliações
- Med Surg 2 - 7 Malabsorption Syndromes and Nursing Care of Clients With Hepatic Disorders 2Documento7 páginasMed Surg 2 - 7 Malabsorption Syndromes and Nursing Care of Clients With Hepatic Disorders 2Maxinne RoseñoAinda não há avaliações
- Amigable, Grant Kenneth D. BSN 3A Define The Disease Causative Agent Signs and Symptoms Nursing Interventions TreatmentDocumento1 páginaAmigable, Grant Kenneth D. BSN 3A Define The Disease Causative Agent Signs and Symptoms Nursing Interventions TreatmentGrant Kenneth Dumo AmigableAinda não há avaliações
- Noninfectious Prostatic Diseases in Dogs: Key FactsDocumento10 páginasNoninfectious Prostatic Diseases in Dogs: Key FactsguadasampaioAinda não há avaliações
- Benign Prostatic Hyperplasia (BPH)Documento26 páginasBenign Prostatic Hyperplasia (BPH)DR-Somalaraju Sateesh Kumar RajuAinda não há avaliações
- Cancer of The ProstateDocumento3 páginasCancer of The ProstateCamille Joy BaliliAinda não há avaliações
- Artigotutoria PDFDocumento12 páginasArtigotutoria PDFZARA BATISTAAinda não há avaliações
- Jurnal Saw PalmettoDocumento3 páginasJurnal Saw PalmettoAde Putri YuliantiAinda não há avaliações
- SL No Content NODocumento12 páginasSL No Content NOPdianghunAinda não há avaliações
- Woldia University College of Health Science For 3 Year HO: Bladder Outflow ObstructionDocumento79 páginasWoldia University College of Health Science For 3 Year HO: Bladder Outflow Obstructionhabtamu tadleAinda não há avaliações
- EAU Pocket On Non Neurogenic Male LUTS 2022Documento26 páginasEAU Pocket On Non Neurogenic Male LUTS 2022AlbalushiAinda não há avaliações
- Benign Prostatic Hyperplasia: Urology Division, Department of Surgery, Faculty of Medicine, University of Sumatera UtaraDocumento38 páginasBenign Prostatic Hyperplasia: Urology Division, Department of Surgery, Faculty of Medicine, University of Sumatera UtaraSalwa Zahra TsamaraAinda não há avaliações
- Ilovepdf Merged 2-69Documento1 páginaIlovepdf Merged 2-69qwivy.comAinda não há avaliações
- Benign Prostatic HyperplasiaDocumento4 páginasBenign Prostatic Hyperplasiaエド パジャロンAinda não há avaliações
- Prostat: Dr. Delyuzar SP - PADocumento66 páginasProstat: Dr. Delyuzar SP - PAJefry SAinda não há avaliações
- Prostate Cancer Clinical Pathway - July 2020Documento4 páginasProstate Cancer Clinical Pathway - July 2020VincentEguzoAinda não há avaliações
- EAU Pocket On Non Neurogenic Male LUTS 2023Documento26 páginasEAU Pocket On Non Neurogenic Male LUTS 2023Norlaila HasbullahAinda não há avaliações
- BPH, Pdui 2017 PDFDocumento36 páginasBPH, Pdui 2017 PDFcyndra erisAinda não há avaliações
- BPH, Pdui 2017Documento36 páginasBPH, Pdui 2017basirAinda não há avaliações
- 17 PDFDocumento10 páginas17 PDFMaríaJosé Palacios CandiaAinda não há avaliações
- Pembahasan Semester 4-5 Maret 2022Documento21 páginasPembahasan Semester 4-5 Maret 2022Angger SatriaAinda não há avaliações
- Diagnosis & Tatalaksana Hipertrofi Prostat Dan Kanker PRDocumento75 páginasDiagnosis & Tatalaksana Hipertrofi Prostat Dan Kanker PRipulAinda não há avaliações
- BPH - TextDocumento7 páginasBPH - TextSomesh GuptaAinda não há avaliações
- Jewett Systems: FrequencyDocumento4 páginasJewett Systems: FrequencysumacumrockersAinda não há avaliações
- Benign Prostatic HyperplasiaDocumento10 páginasBenign Prostatic HyperplasiaRoshwill KingAinda não há avaliações
- A Uro Case2 AlgorithmDocumento1 páginaA Uro Case2 AlgorithmAngelique TongsonAinda não há avaliações
- A2 Prostate Ca - AinDocumento4 páginasA2 Prostate Ca - AinNur Liyana Ahmad ZakiAinda não há avaliações
- Benign Prostatic HyperplasiaDocumento22 páginasBenign Prostatic HyperplasiaMc N Mi Kabiling100% (1)
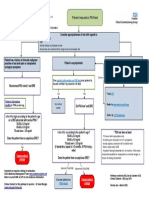
- PSA Pathway: Patient Requests A PSA TestDocumento1 páginaPSA Pathway: Patient Requests A PSA Testaveen rasulAinda não há avaliações
- Accessory OrgansDocumento6 páginasAccessory OrgansNadia AbdurasidAinda não há avaliações
- Bible Chirurgie Schemas-1Documento38 páginasBible Chirurgie Schemas-1Marcel HairmeroAinda não há avaliações
- Health EducationDocumento5 páginasHealth Educationsudeepminz15Ainda não há avaliações
- Amenorrhea: Definition - This Is The Symptom of Absence of MenstruationDocumento10 páginasAmenorrhea: Definition - This Is The Symptom of Absence of MenstruationSuhas IngaleAinda não há avaliações
- Benign Prostatic Hyperplasia: Learning ObjectiveDocumento19 páginasBenign Prostatic Hyperplasia: Learning ObjectiveDeviruchi GamingAinda não há avaliações
- BPH - TextDocumento7 páginasBPH - TextSomesh GuptaAinda não há avaliações
- Benign Prostatic HyperplasiaDocumento22 páginasBenign Prostatic HyperplasiaQueen SofiaAinda não há avaliações
- Cannabis As Cause of Death Drummer2019Documento9 páginasCannabis As Cause of Death Drummer2019yossiAinda não há avaliações
- Mark Scheme (Provisional) Summer 2021: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BDocumento17 páginasMark Scheme (Provisional) Summer 2021: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BThakoon TtsAinda não há avaliações
- Mark Scheme (Results) January 2021: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BRDocumento16 páginasMark Scheme (Results) January 2021: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BRThakoon TtsAinda não há avaliações
- January 2021 P2BR QPDocumento24 páginasJanuary 2021 P2BR QPSareeha SadhviAinda não há avaliações
- Mark Scheme (Provisional) Summer 2021: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BDocumento17 páginasMark Scheme (Provisional) Summer 2021: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BThakoon TtsAinda não há avaliações
- Unger Et Al 2020 2020 International Society of Hypertension Global Hypertension Practice GuidelinesDocumento24 páginasUnger Et Al 2020 2020 International Society of Hypertension Global Hypertension Practice GuidelinesEduardo Marco Villarama DayritAinda não há avaliações
- January 2021 P2BR QPDocumento24 páginasJanuary 2021 P2BR QPSareeha SadhviAinda não há avaliações
- Monday 1 June 2020: BiologyDocumento20 páginasMonday 1 June 2020: BiologyAdeeba iqbal100% (2)
- Mark Scheme (Results) November 2020: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BDocumento19 páginasMark Scheme (Results) November 2020: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BThakoon TtsAinda não há avaliações
- Mark Scheme (Results) January 2021: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BDocumento25 páginasMark Scheme (Results) January 2021: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BThakoon TtsAinda não há avaliações
- Monday 1 June 2020: BiologyDocumento20 páginasMonday 1 June 2020: BiologyAdeeba iqbal100% (2)
- Monday 1 June 2020: BiologyDocumento16 páginasMonday 1 June 2020: BiologyThakoon TtsAinda não há avaliações
- ENT - Diseases of The Inner Ear 2014Documento4 páginasENT - Diseases of The Inner Ear 2014Thakoon TtsAinda não há avaliações
- Mark Scheme (Results) November 2020: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BRDocumento16 páginasMark Scheme (Results) November 2020: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BRThakoon TtsAinda não há avaliações
- Skin & Subcutaneous TissueDocumento10 páginasSkin & Subcutaneous TissueThakoon TtsAinda não há avaliações
- Urinary StoneDocumento5 páginasUrinary StoneThakoon TtsAinda não há avaliações
- Subspec Urology: GU TumorsDocumento5 páginasSubspec Urology: GU TumorsThakoon TtsAinda não há avaliações
- ENT - Dse of Inner EarDocumento7 páginasENT - Dse of Inner EarThakoon TtsAinda não há avaliações
- 13.topical Steroid Usage-2011 PDFDocumento8 páginas13.topical Steroid Usage-2011 PDFThakoon TtsAinda não há avaliações
- PEDIA Neuromuscular DisorderDocumento3 páginasPEDIA Neuromuscular DisorderThakoon TtsAinda não há avaliações
- Antiprotozoal Agents: Pharmacology Group III Beguas, Beltran, Bejawada, Bingari, Cabrera, Cadawas, CaliwagDocumento86 páginasAntiprotozoal Agents: Pharmacology Group III Beguas, Beltran, Bejawada, Bingari, Cabrera, Cadawas, CaliwagThakoon TtsAinda não há avaliações
- Common GI Signs and SymptomsDocumento66 páginasCommon GI Signs and SymptomsThakoon TtsAinda não há avaliações
- Diseases of The Immune SystemDocumento19 páginasDiseases of The Immune SystemThakoon TtsAinda não há avaliações
- EAR Anatomy, Physiology, Embryology & Congenital AnomalyDocumento6 páginasEAR Anatomy, Physiology, Embryology & Congenital AnomalyThakoon TtsAinda não há avaliações
- Common Gi Signs and SymptomsDocumento11 páginasCommon Gi Signs and SymptomsThakoon TtsAinda não há avaliações
- Immune Landscape v11Documento100 páginasImmune Landscape v11onco learnAinda não há avaliações
- Public Speaking ScriptDocumento2 páginasPublic Speaking Scriptsalbinarabi100% (1)
- Moringa OleiferaDocumento4 páginasMoringa Oleiferajap pagharionAinda não há avaliações
- Make A Short DNA ModelDocumento5 páginasMake A Short DNA ModelShashank TiwariAinda não há avaliações
- What Is A Bladder Diverticulum?Documento3 páginasWhat Is A Bladder Diverticulum?luckyariadneeAinda não há avaliações
- Oral Manifestations of Denture AbuseDocumento53 páginasOral Manifestations of Denture AbuseBharanija100% (2)
- Daftar Pustaka SpaDocumento10 páginasDaftar Pustaka SpaRina PratiwiAinda não há avaliações
- Pages 300-331Documento31 páginasPages 300-331aptureinc100% (13)
- Draft Guidelines Housing MiceDocumento136 páginasDraft Guidelines Housing MiceindrieliciousAinda não há avaliações
- Microarray DatabasesDocumento3 páginasMicroarray Databaseswilliam919Ainda não há avaliações
- Wilms Tumor NelsonDocumento8 páginasWilms Tumor NelsonvegaAinda não há avaliações
- Akt RenalDocumento4 páginasAkt Renaldzidek7Ainda não há avaliações
- Etiologic Agents: Laporga, Stephani Grace A. S2ADocumento4 páginasEtiologic Agents: Laporga, Stephani Grace A. S2AMonique Nofuente ZamudioAinda não há avaliações
- HSB QA What Is DigestionDocumento37 páginasHSB QA What Is DigestionVivienne WrightAinda não há avaliações
- Principal of Inheritance Extra Questions and Its HintsDocumento6 páginasPrincipal of Inheritance Extra Questions and Its Hintssunder singhAinda não há avaliações
- Case PresentationDocumento21 páginasCase PresentationMae Alleslie TolentinoAinda não há avaliações
- SOPDocumento2 páginasSOPNIGEL SAANAAinda não há avaliações
- Org - Telegram.messenger - Provider Media Telegram Telegram Documents 4 5985610863455765491 PDFDocumento2 páginasOrg - Telegram.messenger - Provider Media Telegram Telegram Documents 4 5985610863455765491 PDFsameeAinda não há avaliações
- V.I.P. Very Important Points: Dr. Adel Al HarbiDocumento143 páginasV.I.P. Very Important Points: Dr. Adel Al HarbiSukainah AL-AbkaryAinda não há avaliações
- Pharmacogenetics 2022 23Documento52 páginasPharmacogenetics 2022 23Erdem Altun100% (1)