Você também pode gostar
- Claim For Dental Care Expenses: Dentist InformationDocumento2 páginasClaim For Dental Care Expenses: Dentist InformationAbdelbassit Abdessamed SenhadjiAinda não há avaliações
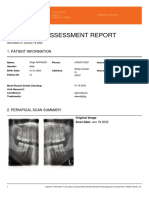
- Periapical Assessment Report: Bright Teeth ClinicDocumento2 páginasPeriapical Assessment Report: Bright Teeth ClinicGaurav SrivastavaAinda não há avaliações
- Dental Chart BSAVADocumento1 páginaDental Chart BSAVAFabiola CabreraAinda não há avaliações
- Su DentalDocumento2 páginasSu DentalMohammed Abdul KhaderAinda não há avaliações
- Periapical Assessment Report: Bright Teeth ClinicDocumento2 páginasPeriapical Assessment Report: Bright Teeth ClinicGaurav SrivastavaAinda não há avaliações
- Dental Charting (Updated)Documento56 páginasDental Charting (Updated)Rose Antoinette Umayam100% (1)
- Network Health EOB Template - SampleDocumento3 páginasNetwork Health EOB Template - SamplePrachi TomarAinda não há avaliações
- Periapical Assessment Report: Bright Teeth ClinicDocumento2 páginasPeriapical Assessment Report: Bright Teeth ClinicGaurav SrivastavaAinda não há avaliações
- Oral Health Examination Record For TNTPDocumento1 páginaOral Health Examination Record For TNTPJellyn Cadorna100% (1)
- Periapical Assessment Report: Bright Teeth ClinicDocumento2 páginasPeriapical Assessment Report: Bright Teeth ClinicGaurav SrivastavaAinda não há avaliações
- Department of Education: Republic of The PhilippinesDocumento1 páginaDepartment of Education: Republic of The PhilippinesLicca ArgallonAinda não há avaliações
- Med 2Documento2 páginasMed 2api-259279833Ainda não há avaliações
- E 355Documento10 páginasE 355Nidhi JayanAinda não há avaliações
- Oral Health Examination Record For Teachers and Non-Teaching PersonnelDocumento3 páginasOral Health Examination Record For Teachers and Non-Teaching PersonnelDaisy's Home Cooking100% (6)
- Dental Health Record Teaching and Non-Teaching Personnel: Index: DMFTDocumento2 páginasDental Health Record Teaching and Non-Teaching Personnel: Index: DMFTEmerson NunezAinda não há avaliações
- Patient Encounter Form: Facility Number: Facility Name: Facility Address: NPI NumberDocumento2 páginasPatient Encounter Form: Facility Number: Facility Name: Facility Address: NPI NumberJayAinda não há avaliações
- EXC-MBR-MDM-EMP-BKR-Dental Claim FormDocumento2 páginasEXC-MBR-MDM-EMP-BKR-Dental Claim Formnicholas beehnerAinda não há avaliações
- 101 102 201 202 103 104 105 106 107 108 109 110 RHS 411 410 203 204 205 206 207 208 209 210 LHS 311 310 409 309 408 308 407 307Documento2 páginas101 102 201 202 103 104 105 106 107 108 109 110 RHS 411 410 203 204 205 206 207 208 209 210 LHS 311 310 409 309 408 308 407 307Vadim DonchenkoAinda não há avaliações
- And The Tooth Cracked PDFDocumento21 páginasAnd The Tooth Cracked PDFHector Flores SotoAinda não há avaliações
- And The Tooth CrackedDocumento20 páginasAnd The Tooth Crackedpablogdv956Ainda não há avaliações
- USDA Forest Service Floating Trail Bridges and DocksDocumento31 páginasUSDA Forest Service Floating Trail Bridges and DocksRockWagonAinda não há avaliações
- Claim Form - Dentacare: 1. Patient'S DetailsDocumento3 páginasClaim Form - Dentacare: 1. Patient'S DetailsSivaramanAinda não há avaliações
- PG Dental Fee and Seat 2020Documento1 páginaPG Dental Fee and Seat 2020Saurav SumanAinda não há avaliações
- Application IagdDocumento3 páginasApplication IagdUsha KiranAinda não há avaliações
- Malm Gren 1982Documento5 páginasMalm Gren 1982michele_ronquilloAinda não há avaliações
- Treatment of Child With Four Lost Maxillary Incisors Due To Traffic InjuryDocumento10 páginasTreatment of Child With Four Lost Maxillary Incisors Due To Traffic InjuryOana DimaAinda não há avaliações
- Premaxilla Excess CleftDocumento7 páginasPremaxilla Excess CleftDean Faculty of DentistryAinda não há avaliações
- CDH June11 2552-Bartlett Pp182-187Documento6 páginasCDH June11 2552-Bartlett Pp182-187qzd6nnrpptAinda não há avaliações
- Oral & Maxillofacial Surgery, Inc.: 03/15/2023 Cailey Rubin 03/13/2001 Kenneth Rubin Cpr3313@gmail - OmDocumento1 páginaOral & Maxillofacial Surgery, Inc.: 03/15/2023 Cailey Rubin 03/13/2001 Kenneth Rubin Cpr3313@gmail - Omcailey RubinAinda não há avaliações
- Activity 3Documento3 páginasActivity 3JetAinda não há avaliações
- Asymptomatic Radiopacity of Mandible Causing Delayed Orthodontic Tooth Movement: A Case ReportDocumento4 páginasAsymptomatic Radiopacity of Mandible Causing Delayed Orthodontic Tooth Movement: A Case ReportDiana RizkiAinda não há avaliações
- AXA Dental Claim FormDocumento2 páginasAXA Dental Claim FormDaren OngAinda não há avaliações
- WarningDocumento1 páginaWarningbjluevwsakyotmhyjwAinda não há avaliações
- Oral Health Examination RecordDocumento1 páginaOral Health Examination RecordJefrey N. Gonzales100% (1)
- QT-211016836 Revised 1Documento1 páginaQT-211016836 Revised 1mabel lowAinda não há avaliações
- Mohammed Almogalli ResumeDocumento2 páginasMohammed Almogalli Resumeapi-660195097Ainda não há avaliações
- Liberty Referral PDFDocumento1 páginaLiberty Referral PDFTuba HabibAinda não há avaliações
- A New Look at Erosive Tooth WearDocumento5 páginasA New Look at Erosive Tooth WearfarahAinda não há avaliações
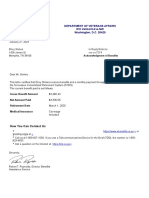
- ElroyStokes Acknowledgment Is It Right Now Acknowledgment Anything of BenefitsDocumento1 páginaElroyStokes Acknowledgment Is It Right Now Acknowledgment Anything of BenefitsMik JrAinda não há avaliações
- Preface Oralandcraniofacialimplant Reconstructionasfoundation ForrestorativedentistryDocumento1 páginaPreface Oralandcraniofacialimplant Reconstructionasfoundation ForrestorativedentistryKranti PrajapatiAinda não há avaliações
- QT 220633619Documento1 páginaQT 220633619mabel lowAinda não há avaliações
- Dental CodingDocumento74 páginasDental CodingSakshi Bishnoi100% (2)
- RCG SoaDocumento1 páginaRCG Soaraymon generAinda não há avaliações
- Oral Health Examination RecordDocumento2 páginasOral Health Examination Recordeugene.camahinAinda não há avaliações
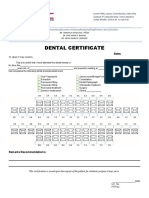
- Dental CertificateDocumento1 páginaDental CertificateNicole Antolijao PiñonAinda não há avaliações
- School ForpolioDocumento7 páginasSchool ForpolioJuzzel Edward ConcepcionAinda não há avaliações
- Adobe Scan Jan 9, 2024Documento1 páginaAdobe Scan Jan 9, 2024ebrima.koitaAinda não há avaliações
- Dental Claim FormDocumento2 páginasDental Claim Formbleung123Ainda não há avaliações
- Telus Donation - March 2011Documento2 páginasTelus Donation - March 2011Richmond Association for MontessoriAinda não há avaliações
- Dental Microscope For General DentistryDocumento3 páginasDental Microscope For General DentistrylupusebastianAinda não há avaliações
- TIET (Fee Confirmation SlipDocumento1 páginaTIET (Fee Confirmation SlipSimranjotSinghAinda não há avaliações
- Esthetic Rehabilitation of Tetracycline-Stained and Worn Teeth With Porcelain Laminate VeneersDocumento8 páginasEsthetic Rehabilitation of Tetracycline-Stained and Worn Teeth With Porcelain Laminate VeneersunsospiroAinda não há avaliações
- 101 102 201 202 103 104 106 107 108 109 RHS 203 204 206 207 208 209 LHSDocumento2 páginas101 102 201 202 103 104 106 107 108 109 RHS 203 204 206 207 208 209 LHSVadim DonchenkoAinda não há avaliações
- Oral Health Examination Record For Teaching and Non-Teaching PersonnelDocumento6 páginasOral Health Examination Record For Teaching and Non-Teaching PersonnelCarmela BlanquerAinda não há avaliações
- Ribbond For Treatment of Complicated Crown Fractures: Report of 3 CasesDocumento4 páginasRibbond For Treatment of Complicated Crown Fractures: Report of 3 CasesAmmyAinda não há avaliações
- Tts SplintDocumento5 páginasTts SplintanatomimanusiaAinda não há avaliações
- Clark and Khadem IDocumento10 páginasClark and Khadem IRam sharmaAinda não há avaliações
- Disaster Victim Management: Role of Forensic Odontology: GlossaryDocumento17 páginasDisaster Victim Management: Role of Forensic Odontology: GlossaryFlorin UngureanuAinda não há avaliações
- 0008a 08 11 Fs Web RV 09 18-1Documento3 páginas0008a 08 11 Fs Web RV 09 18-1OvadoseAinda não há avaliações
- Manoshe Street Takeaway MenuDocumento9 páginasManoshe Street Takeaway MenuimaddakrAinda não há avaliações
- HSE Issues Tracker - DAFDocumento28 páginasHSE Issues Tracker - DAFMohd Abdul MujeebAinda não há avaliações
- Made in His ImageThe Amazing Design of The Human BodyDocumento4 páginasMade in His ImageThe Amazing Design of The Human BodyAriam MariaAinda não há avaliações
- Lecture 16 - Bleeding Tendency DiseasesDocumento64 páginasLecture 16 - Bleeding Tendency Diseasesapi-3703352100% (1)
- Ielts TASK 1 ExerciseDocumento3 páginasIelts TASK 1 Exerciseanitha nathenAinda não há avaliações
- Tutorial 2 Organizing DataDocumento2 páginasTutorial 2 Organizing Datazurila zakariaAinda não há avaliações
- Silicon Epitaxial Planar Transistor 2SA1179: Galaxy ElectricalDocumento5 páginasSilicon Epitaxial Planar Transistor 2SA1179: Galaxy ElectricalsacralAinda não há avaliações
- 1198-Article Text-5716-1-10-20221219Documento9 páginas1198-Article Text-5716-1-10-20221219Hendarko AriAinda não há avaliações
- Itopride HCL Pynetic 50mg TabDocumento2 páginasItopride HCL Pynetic 50mg TabAusaf AhmadAinda não há avaliações
- Tinda Tomato PachadiDocumento1 páginaTinda Tomato PachadijyosriAinda não há avaliações
- 1716 ch05Documento103 páginas1716 ch05parisliuhotmail.comAinda não há avaliações
- Hindustan Coca-Cola Beverages PVT LTD B-91 Mayapuri Industrial Area Phase-I New DelhiDocumento2 páginasHindustan Coca-Cola Beverages PVT LTD B-91 Mayapuri Industrial Area Phase-I New DelhiUtkarsh KadamAinda não há avaliações
- PM PillarDocumento56 páginasPM PillarNavneet Sharma75% (4)
- 65 70Documento6 páginas65 70kang soon cheolAinda não há avaliações
- Shutdown Jobs List C & IDocumento12 páginasShutdown Jobs List C & Imanohar kumar0% (1)
- OSA Winter 2011 NewsletterDocumento18 páginasOSA Winter 2011 NewsletterNABSWOSAAinda não há avaliações
- Lean Six Sigma Green BeltDocumento7 páginasLean Six Sigma Green Beltmulpuru sai snehaAinda não há avaliações
- Pizza Hut and Dominos - A Comparative AnalysisDocumento19 páginasPizza Hut and Dominos - A Comparative AnalysisSarvesh Kumar GautamAinda não há avaliações
- Client Travel Policy Guidelines Nunavut Health Care PlanDocumento8 páginasClient Travel Policy Guidelines Nunavut Health Care PlanNunatsiaqNewsAinda não há avaliações
- Parreira CVDocumento8 páginasParreira CVapi-595476865Ainda não há avaliações
- Mycesmm2 Quiz: Please Circle Your Answer! Time Allocated To Answer Is 30 MinutesDocumento2 páginasMycesmm2 Quiz: Please Circle Your Answer! Time Allocated To Answer Is 30 MinutesSi Qian LuiAinda não há avaliações
- Mount Kenya University: Department: School of Social SciencesDocumento4 páginasMount Kenya University: Department: School of Social SciencesLETISIA FATUMAAinda não há avaliações
- Kuan Yin Prayer Book.Documento11 páginasKuan Yin Prayer Book.AddySuBa85% (13)
- Identification of Plastics Identification of PlasticsDocumento41 páginasIdentification of Plastics Identification of PlasticsSoumickAinda não há avaliações
- AnswersDocumento4 páginasAnswersamitmehta29Ainda não há avaliações
- "Mode One" Author & Dating Coach Alan Roger Currie Releases Criticism of Alleged Harvey Weinstein BehaviorDocumento3 páginas"Mode One" Author & Dating Coach Alan Roger Currie Releases Criticism of Alleged Harvey Weinstein BehaviorPR.com100% (1)
- Easy Exercises For Hip Flexor PainDocumento1 páginaEasy Exercises For Hip Flexor PainJackieAinda não há avaliações
- Tolerance Chart: (Maximum Permissible Error)Documento3 páginasTolerance Chart: (Maximum Permissible Error)arif_setyaw4nAinda não há avaliações
- 1-1FlowCharts For HaccpDocumento3 páginas1-1FlowCharts For HaccpPeter George0% (1)
- Instructions For Assembling Your Owners ManualDocumento8 páginasInstructions For Assembling Your Owners ManualJim PowersAinda não há avaliações