Você também pode gostar
- Analogue Electronics: - Operational AmplifiersDocumento46 páginasAnalogue Electronics: - Operational AmplifiersNimsiri AbhayasingheAinda não há avaliações
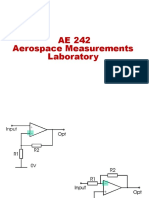
- AE 242 Aerospace Measurements LaboratoryDocumento23 páginasAE 242 Aerospace Measurements LaboratoryAnubhavAinda não há avaliações
- Operational Amplifiers: Chapter-1Documento45 páginasOperational Amplifiers: Chapter-1meseret sisayAinda não há avaliações
- AE 242 Aerospace Measurements LaboratoryDocumento41 páginasAE 242 Aerospace Measurements LaboratoryAnubhavAinda não há avaliações
- Introduction To Op Amp Circuits: ECEM325Documento32 páginasIntroduction To Op Amp Circuits: ECEM325Sean Joshua CarilloAinda não há avaliações
- Introduction To Op-Amp PDFDocumento23 páginasIntroduction To Op-Amp PDFJeswant TSAinda não há avaliações
- Operational Amplifiers: Brandon Borm Shelley Nation Chloe MilionDocumento33 páginasOperational Amplifiers: Brandon Borm Shelley Nation Chloe MilionrakibAinda não há avaliações
- ECE131 UNIT5 Part3Documento88 páginasECE131 UNIT5 Part3abhi shek100% (1)
- Physical Limitations of Op AmpsDocumento18 páginasPhysical Limitations of Op AmpsFabricio AlvarezAinda não há avaliações
- Eee 1217 Op AmpDocumento51 páginasEee 1217 Op AmpEbrahim SiddikAinda não há avaliações
- Unit-IV - OP-AMP and Its ApplicationsDocumento64 páginasUnit-IV - OP-AMP and Its ApplicationsJadhav BhagavatAinda não há avaliações
- Operational AmplifiersDocumento56 páginasOperational AmplifiersRupert Rosel AmatorioAinda não há avaliações
- Linear & Digital IcDocumento282 páginasLinear & Digital IcdigitalromAinda não há avaliações
- L2 - Operational AmplifiersDocumento22 páginasL2 - Operational AmplifiersHanan ShayiboAinda não há avaliações
- Operational Amplifiers: David Lomax Azeem Meruani Gautam JadhavDocumento28 páginasOperational Amplifiers: David Lomax Azeem Meruani Gautam JadhavJaideep SinghAinda não há avaliações
- Operational Amplifiers: David Lomax Azeem Meruani Gautam JadhavDocumento28 páginasOperational Amplifiers: David Lomax Azeem Meruani Gautam JadhavSrijan ThakurAinda não há avaliações
- CH 2 - Op-Amp ApplicationDocumento52 páginasCH 2 - Op-Amp Applicationknighthood4all100% (2)
- Operational Amplifiers and ApplicationsDocumento47 páginasOperational Amplifiers and Applicationsilias ahmedAinda não há avaliações
- Ic NotesDocumento67 páginasIc NotesVijaya Kumar VadladiAinda não há avaliações
- 5.2) (2) AmplifierDocumento63 páginas5.2) (2) AmplifierJuan Felipe LeyvaAinda não há avaliações
- محاضره 3Documento51 páginasمحاضره 3Safwan HadiAinda não há avaliações
- Chapter 10Documento18 páginasChapter 10Nasser AlmofariAinda não há avaliações
- Lic Unit 1 (1) eDocumento114 páginasLic Unit 1 (1) eganeshAinda não há avaliações
- Op-Amps: and Why They Are Useful To UsDocumento32 páginasOp-Amps: and Why They Are Useful To UsUmaAinda não há avaliações
- Electronics Analog OPAMPDocumento51 páginasElectronics Analog OPAMPPrashant SachdevAinda não há avaliações
- Ecd Lec-1-2Documento37 páginasEcd Lec-1-2assad abidAinda não há avaliações
- OpAmp F10Documento32 páginasOpAmp F10Suguna PriyaAinda não há avaliações
- Opamp ApplicationDocumento38 páginasOpamp ApplicationS.m. FerdousAinda não há avaliações
- EE 220 Chap 4 DraftDocumento23 páginasEE 220 Chap 4 DraftomAinda não há avaliações
- Operational AmplifiersDocumento33 páginasOperational Amplifiersaayush kumar nayakAinda não há avaliações
- QB105452Documento6 páginasQB105452Sridarshini VikkramAinda não há avaliações
- Electronic Instrumentation: Experiment 4Documento63 páginasElectronic Instrumentation: Experiment 4helenarajAinda não há avaliações
- Opamp Problems 2Documento11 páginasOpamp Problems 2علي جليلAinda não há avaliações
- Op AmpDocumento57 páginasOp AmpDivyanshu Yadav100% (1)
- Operational Amplifiers: Building Blocks of ServosDocumento12 páginasOperational Amplifiers: Building Blocks of ServosArvind SinghAinda não há avaliações
- Introduction To AmplifiersDocumento25 páginasIntroduction To Amplifiersrahul prasadAinda não há avaliações
- Ideal Op-Amps and Basic Circuits (Autosaved)Documento49 páginasIdeal Op-Amps and Basic Circuits (Autosaved)Stephanus AbednegoAinda não há avaliações
- EMT 359/3 Analog Electronic II: Op-Amp Applications & Frequency ResponseDocumento59 páginasEMT 359/3 Analog Electronic II: Op-Amp Applications & Frequency ResponsedharanikaAinda não há avaliações
- OPAMPDocumento24 páginasOPAMPEr Akhilesh SinghAinda não há avaliações
- Op Amp Electronics Lab ReportDocumento4 páginasOp Amp Electronics Lab ReportBushra MamoudAinda não há avaliações
- EE 174 Fall 2019: Operational AmplifiersDocumento36 páginasEE 174 Fall 2019: Operational AmplifiersKavyashreeMAinda não há avaliações
- Operational Amplifier and Its Applications: Unit 5Documento20 páginasOperational Amplifier and Its Applications: Unit 5Chiraag ChiruAinda não há avaliações
- Unit 5 Op Amp NewDocumento24 páginasUnit 5 Op Amp NewAkram MohithAinda não há avaliações
- Feedback Amplifiers: Electronic Circuit IIDocumento55 páginasFeedback Amplifiers: Electronic Circuit IIDeepa RangasamyAinda não há avaliações
- Presentation Op Amp Till 16.01.2024Documento32 páginasPresentation Op Amp Till 16.01.2024Harsh AgarwalAinda não há avaliações
- Ch7 Operational Amplifiers and Op Amp CircuitsDocumento92 páginasCh7 Operational Amplifiers and Op Amp CircuitsBagus dwiAinda não há avaliações
- 03 Analog Electronics-IIDocumento63 páginas03 Analog Electronics-IINazmus SakibAinda não há avaliações
- Unit 2 - Operational AmplifiersDocumento32 páginasUnit 2 - Operational AmplifiersVimala ElumalaiAinda não há avaliações
- Operational Amplifier: Shubha Gokhale School of Sciences, IGNOUDocumento35 páginasOperational Amplifier: Shubha Gokhale School of Sciences, IGNOUKRISHNAVINODAinda não há avaliações
- 15EE46 Notes Module-1Documento7 páginas15EE46 Notes Module-1jagavannammaAinda não há avaliações
- Analog & Digital Electronics: Course No: PH-218 Lec-23: Operational AmplifiersDocumento14 páginasAnalog & Digital Electronics: Course No: PH-218 Lec-23: Operational AmplifiersAli Hasan SifatAinda não há avaliações
- Chap5 BEKG1113Documento30 páginasChap5 BEKG1113am2030Ainda não há avaliações
- Operational Amplifier PDFDocumento45 páginasOperational Amplifier PDFAnonymous H6zpNuAinda não há avaliações
- 2020 IK OpAmpDocumento26 páginas2020 IK OpAmpAdi Kurniawan EffendiAinda não há avaliações
- Microelectronics: Circuit Analysis and Design Donald A. NeamenDocumento12 páginasMicroelectronics: Circuit Analysis and Design Donald A. NeamenBhandari PrakashAinda não há avaliações
- LM358 Op AmpDocumento7 páginasLM358 Op AmpRuang OtomasiAinda não há avaliações
- WEEK 5 - CHAPTER 3.pdf Electronic CircuitDocumento38 páginasWEEK 5 - CHAPTER 3.pdf Electronic CircuitChris DannyAinda não há avaliações
- Unit 3 OpampDocumento64 páginasUnit 3 Opamprudranshvsingh4705Ainda não há avaliações
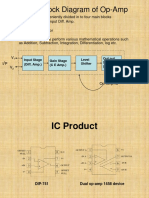
- Basic Block Diagram of Op-Amp: Input Stage (Diff. Amp.) Gain Stage (C E Amp.) Level Shifter Out Put Stage (Buffer)Documento26 páginasBasic Block Diagram of Op-Amp: Input Stage (Diff. Amp.) Gain Stage (C E Amp.) Level Shifter Out Put Stage (Buffer)Pierana PolitaniAinda não há avaliações
- Refrigeration and Air ConditioningDocumento10 páginasRefrigeration and Air ConditioningSamama khanAinda não há avaliações
- Class MD 6 SpurGears PDFDocumento58 páginasClass MD 6 SpurGears PDFSamama khanAinda não há avaliações
- Bevel GearDocumento22 páginasBevel GearSamama khan100% (1)
- Assignment No. 2: Problems: 15, 16, 20 - Chapter No. 1 - Page # 111 To 113Documento1 páginaAssignment No. 2: Problems: 15, 16, 20 - Chapter No. 1 - Page # 111 To 113Samama khanAinda não há avaliações
- Iphone 6 Plus 5.5'' 820-3675 051-0517 N56 MLB Rev 6.0.0 - 05.09.2014 Schematic DiagramDocumento55 páginasIphone 6 Plus 5.5'' 820-3675 051-0517 N56 MLB Rev 6.0.0 - 05.09.2014 Schematic DiagramJose Perez GarciaAinda não há avaliações
- Module-Hands Free C1Documento2 páginasModule-Hands Free C1Halit KorpeAinda não há avaliações
- Networking AssignmentDocumento37 páginasNetworking AssignmentTerry HalAinda não há avaliações
- DICA Lab Manual PDFDocumento36 páginasDICA Lab Manual PDFusharaniAinda não há avaliações
- EE525 2014F FinalExamDocumento8 páginasEE525 2014F FinalExamAkinbode Sunday Oluwagbenga100% (1)
- PendriveDocumento6 páginasPendriveSubodh SonawaneAinda não há avaliações
- VectaStar PMPDocumento236 páginasVectaStar PMPevashihminaAinda não há avaliações
- Scalability Analysis of Large-Scale Lorawan Networks in Ns-3Documento12 páginasScalability Analysis of Large-Scale Lorawan Networks in Ns-3Pedrito OrangeAinda não há avaliações
- ZTE Proposed IP Metro Solution For Aftel V 2.0Documento24 páginasZTE Proposed IP Metro Solution For Aftel V 2.0mujibrahmanAinda não há avaliações
- Iptv STB Manual Zxv10 b720Documento2 páginasIptv STB Manual Zxv10 b720disepyAinda não há avaliações
- Assignment 1: Implementation of A Processor (10marks) : Constant RDST OpcodeDocumento6 páginasAssignment 1: Implementation of A Processor (10marks) : Constant RDST OpcodeTharakram KorripatiAinda não há avaliações
- 13142833663.5.6 DCVG Equipment Rev 1Documento2 páginas13142833663.5.6 DCVG Equipment Rev 1ilublessingAinda não há avaliações
- Rule Breakers FinalDocumento22 páginasRule Breakers Finalnello80Ainda não há avaliações
- DHI-KTA02: Video Intercom KitDocumento2 páginasDHI-KTA02: Video Intercom KitÁngel GóticoAinda não há avaliações
- How To Configure Tvheadend For DVB Tuner PDFDocumento8 páginasHow To Configure Tvheadend For DVB Tuner PDFRafa AguileraAinda não há avaliações
- Omnitron Catalog 2014Documento58 páginasOmnitron Catalog 2014Anonymous nC9gpUWPAinda não há avaliações
- Trouble Memo Report No.025 - TL 230kV BlackoutDocumento14 páginasTrouble Memo Report No.025 - TL 230kV BlackoutLove Buddha's WordsAinda não há avaliações
- 01 ETR300R Manual Control Ver1.47 201304Documento313 páginas01 ETR300R Manual Control Ver1.47 201304chiemenx100% (1)
- A - Theory - Course Diary - Odd Semester - 2022 - 23 - Google Forms-1Documento4 páginasA - Theory - Course Diary - Odd Semester - 2022 - 23 - Google Forms-1Anikendu MaitraAinda não há avaliações
- EE 442 642 Diode RectifiersDocumento17 páginasEE 442 642 Diode RectifiersKeyboardMan1960Ainda não há avaliações
- Holographic Beamforming WP v.6C FINALDocumento8 páginasHolographic Beamforming WP v.6C FINALsameerAinda não há avaliações
- Festo Products For Your Everyday Automation NeedsDocumento7 páginasFesto Products For Your Everyday Automation NeedsDeddy TandraAinda não há avaliações
- Mindwave Mobile & ArduinoDocumento12 páginasMindwave Mobile & ArduinoMuhammad Shafiq Abdul KarimAinda não há avaliações
- Usb Communication Cable 750-923Documento7 páginasUsb Communication Cable 750-923Malek MessaoudAinda não há avaliações
- 2.1 Channel Soundbar With Wireless Subwoofer: Instruction ManualDocumento28 páginas2.1 Channel Soundbar With Wireless Subwoofer: Instruction ManualKarloof AutencioAinda não há avaliações
- Simpledsp: A Fast and Flexible DSP Processor Model: (Extended Abstract)Documento6 páginasSimpledsp: A Fast and Flexible DSP Processor Model: (Extended Abstract)Alex ObrejanAinda não há avaliações
- Ipasolink Series: System OverviewDocumento69 páginasIpasolink Series: System Overviewธนวรรณ โภคาอนนต์100% (3)
- PDFDocumento2 páginasPDFHassanAhmed100% (1)
- M29F400T M29F400B: 4 Mbit (512Kb x8 or 256Kb x16, Boot Block) Single Supply Flash MemoryDocumento34 páginasM29F400T M29F400B: 4 Mbit (512Kb x8 or 256Kb x16, Boot Block) Single Supply Flash MemorykokotnoAinda não há avaliações
- TelcoBriges SS7 Spec SheetDocumento2 páginasTelcoBriges SS7 Spec Sheetapi-3833851Ainda não há avaliações