Você também pode gostar
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Assessment Clo1 Clo2 Clo3 Clo4 Clo5 Plo1 Plo2 Plo2 Plo1Documento12 páginasAssessment Clo1 Clo2 Clo3 Clo4 Clo5 Plo1 Plo2 Plo2 Plo1Ma Liu Hun VuiAinda não há avaliações
- Wireless Mouse m325 Quick Start GuideDocumento2 páginasWireless Mouse m325 Quick Start GuideFabolos 9Ainda não há avaliações
- Minor Project Report On Efficiency Improvement of A Combined Cycle Power PlantDocumento40 páginasMinor Project Report On Efficiency Improvement of A Combined Cycle Power PlantArpit Garg100% (1)
- How Do We Classify An Antipumping Relay?: What Will Happen If Antipumping Relay Circuit Is Not Present?Documento6 páginasHow Do We Classify An Antipumping Relay?: What Will Happen If Antipumping Relay Circuit Is Not Present?joseAinda não há avaliações
- TV Compatibility with Verbatim HDDsDocumento2 páginasTV Compatibility with Verbatim HDDsmirciulicacatyAinda não há avaliações
- Experion Scada PinDocumento7 páginasExperion Scada PinKhalid AliAinda não há avaliações
- The Synergies of Hybridizing CNC and Additive ManufacturingDocumento8 páginasThe Synergies of Hybridizing CNC and Additive ManufacturingdemuxAinda não há avaliações
- Nature of Acidity and Lime Requirement in Acid Soils of ManipurDocumento8 páginasNature of Acidity and Lime Requirement in Acid Soils of ManipurIJASRETAinda não há avaliações
- CH (1) : Introduction: 1.1: Database Management SystemsDocumento5 páginasCH (1) : Introduction: 1.1: Database Management SystemsaboalfotohAinda não há avaliações
- Directional OCDocumento301 páginasDirectional OCurcalmAinda não há avaliações
- Dow Corning (R) 200 Fluid, 50 Cst.Documento11 páginasDow Corning (R) 200 Fluid, 50 Cst.Sergio Gonzalez GuzmanAinda não há avaliações
- CompoundingDocumento5 páginasCompoundingMajester RigsAinda não há avaliações
- Sinusverteiler Multivalent SolutionsDocumento13 páginasSinusverteiler Multivalent SolutionsIon ZabetAinda não há avaliações
- Communication System (LC-ECE204G) LAB ManualDocumento54 páginasCommunication System (LC-ECE204G) LAB ManualBindia HandaAinda não há avaliações
- AMS Thread Size ChartDocumento4 páginasAMS Thread Size Chartarunvelu_1250% (2)
- CV Enric Durany enDocumento2 páginasCV Enric Durany enenricduranyAinda não há avaliações
- Generation of Electrical Energy - B. R. GuptaDocumento171 páginasGeneration of Electrical Energy - B. R. GuptaIbrahim Ahmed43% (23)
- Customer Targeted E-CommerceDocumento4 páginasCustomer Targeted E-CommercepriyaAinda não há avaliações
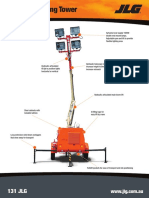
- JLG Lighting Tower 6308AN Series II 20150907Documento2 páginasJLG Lighting Tower 6308AN Series II 20150907DwiSulistyo09Ainda não há avaliações
- Sodium Citrate AUDocumento3 páginasSodium Citrate AUKrishna OgotAinda não há avaliações
- Inventory Management PreetDocumento28 páginasInventory Management PreetKawalpreet Singh MakkarAinda não há avaliações
- ISO 9001 ChecklistDocumento3 páginasISO 9001 Checklistthanh571957Ainda não há avaliações
- Chapter 2 Cast IronDocumento9 páginasChapter 2 Cast IronHelen AdugnaAinda não há avaliações
- Estimating/ Construction Planning/ Scheduling and Programming/ Feasibility Project StudiesDocumento4 páginasEstimating/ Construction Planning/ Scheduling and Programming/ Feasibility Project StudiesVholts Villa VitugAinda não há avaliações
- 02 - Critical Customers Complains enDocumento8 páginas02 - Critical Customers Complains enKJDNKJZEF100% (1)
- Catalog Advantys AS-I IP20-IP67 - 803510 - DIA3ED2040909EN - 200408Documento30 páginasCatalog Advantys AS-I IP20-IP67 - 803510 - DIA3ED2040909EN - 200408Jean MarzanAinda não há avaliações
- Ceramic Terminal BlocksDocumento1 páginaCeramic Terminal BlockselijbbAinda não há avaliações
- Feed Water and Boiler Water of Steam GeneratorsDocumento2 páginasFeed Water and Boiler Water of Steam GeneratorsIvicaT0% (2)
- GRI 20RS-12-B Data SheetDocumento6 páginasGRI 20RS-12-B Data SheetJMAC SupplyAinda não há avaliações
- WPD Flotationdrying PDFDocumento19 páginasWPD Flotationdrying PDFVvbjAinda não há avaliações