Você também pode gostar
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Premarital Sex by Group 1Documento1 páginaPremarital Sex by Group 1Rhoda Rose LimAinda não há avaliações
- Motivation and Cognition in ClassroomDocumento34 páginasMotivation and Cognition in ClassroomLo LoloAinda não há avaliações
- Movie ReflectionDocumento4 páginasMovie Reflectionaibajo2004Ainda não há avaliações
- Marzookh CVDocumento2 páginasMarzookh CVmarzookjAinda não há avaliações
- 12 Delay of GratificationDocumento20 páginas12 Delay of GratificationliginaayudiaAinda não há avaliações
- A Discussion On The User Intention of Golfers Toward Golf GPS NavigationDocumento14 páginasA Discussion On The User Intention of Golfers Toward Golf GPS Navigationvaishnavi remmaAinda não há avaliações
- Comparison and ContrastDocumento4 páginasComparison and ContrastSholawaty JoAinda não há avaliações
- The Social Case Work Toward In-Depth HelpingDocumento2 páginasThe Social Case Work Toward In-Depth HelpingDon LiongsonAinda não há avaliações
- Work Smarter, Not Harder: A Final ReflectionDocumento7 páginasWork Smarter, Not Harder: A Final ReflectionAllisonAinda não há avaliações
- Entrepreneurship Development (22032)Documento79 páginasEntrepreneurship Development (22032)Nilesh KallurAinda não há avaliações
- Social Psychology (Psyc 336) Independent Study Section - Fall 2013Documento6 páginasSocial Psychology (Psyc 336) Independent Study Section - Fall 2013Office AcadAinda não há avaliações
- Jocelyn L. Reyes Hrmo: Commission On Human Rights of The PhilippinesDocumento6 páginasJocelyn L. Reyes Hrmo: Commission On Human Rights of The PhilippinesZaigzaagAinda não há avaliações
- Dyad Activity 2Documento4 páginasDyad Activity 2therese angelieAinda não há avaliações
- Teaching and Teacher Education: Maria TulisDocumento13 páginasTeaching and Teacher Education: Maria TulisRubén Páez DíazAinda não há avaliações
- Lesson 1B Community ImmersionDocumento15 páginasLesson 1B Community ImmersionRee April CabalanAinda não há avaliações
- Topics: InstructionDocumento4 páginasTopics: InstructionJoan PulidoAinda não há avaliações
- Gestalt 2Documento25 páginasGestalt 2Astro Counselor Karan100% (1)
- A Summary of Georges PouletDocumento2 páginasA Summary of Georges PouletHai WangAinda não há avaliações
- OT 1025 - Frame of ReferenceDocumento28 páginasOT 1025 - Frame of ReferenceRidz FAinda não há avaliações
- Transfer of Training TheoryDocumento22 páginasTransfer of Training TheorySreya RAinda não há avaliações
- CDR Questionnaire Form: of The Project I.E. How The Objectives of The Project Was Accomplished in Brief.)Documento2 páginasCDR Questionnaire Form: of The Project I.E. How The Objectives of The Project Was Accomplished in Brief.)NASEER AHMAD100% (1)
- Lesson 6 - Egoism and HedonismDocumento18 páginasLesson 6 - Egoism and Hedonismjaja riveraAinda não há avaliações
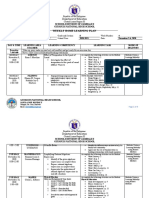
- Weekly Home Learning Plan: Schools Division of Zambales Guisguis National High SchoolDocumento9 páginasWeekly Home Learning Plan: Schools Division of Zambales Guisguis National High SchoolNhatz Gallosa MarticioAinda não há avaliações
- Understanding The SelfDocumento4 páginasUnderstanding The SelfMely SulasulaAinda não há avaliações
- Delos Reyes HTP CHNDocumento5 páginasDelos Reyes HTP CHNEyanah Delos ReyesAinda não há avaliações
- The Paper Mirror: Understanding Reflective Journaling: Delaura L. Hubbs and Charles F. BrandDocumento12 páginasThe Paper Mirror: Understanding Reflective Journaling: Delaura L. Hubbs and Charles F. BrandDhia Aini FatimahAinda não há avaliações
- Updatedct898 Jellison Caep1Documento7 páginasUpdatedct898 Jellison Caep1api-367504817Ainda não há avaliações
- Sedona Method - QuestionsDocumento8 páginasSedona Method - Questionsalle_72100% (7)
- CHPTR 4 PSTMLS Determinants of LearningDocumento8 páginasCHPTR 4 PSTMLS Determinants of LearningBea Reen BurgosAinda não há avaliações
- Project-Based Learning (PJBL) in Three Southeastern Public SchoolDocumento32 páginasProject-Based Learning (PJBL) in Three Southeastern Public SchoolMuhammad YusufAinda não há avaliações