Você também pode gostar
- Treatment of Hypertension-Zanidip 5 Aug 2017 DR Antonia Rev For SlideDocumento31 páginasTreatment of Hypertension-Zanidip 5 Aug 2017 DR Antonia Rev For SlidejoshuaAinda não há avaliações
- Anupam AnandDocumento1 páginaAnupam AnandTuhinaRajAinda não há avaliações
- HTN managment-JNC7Documento37 páginasHTN managment-JNC7Vaibhav KaroliyaAinda não há avaliações
- Efficacy of Beta - Blockers For First - Line Antihypertensive All Beta - Blockers Same?Documento70 páginasEfficacy of Beta - Blockers For First - Line Antihypertensive All Beta - Blockers Same?Kishan Seth100% (1)
- Beta BlockersDocumento70 páginasBeta BlockersIrina Cabac-PogoreviciAinda não há avaliações
- Lower Is Better - FinalDocumento91 páginasLower Is Better - FinalJamsidul Hassan RajibAinda não há avaliações
- Aha Guidelinedriven Management of Hypertension An Evidencebased UpdateDocumento56 páginasAha Guidelinedriven Management of Hypertension An Evidencebased UpdateNanda Gopal Reddy AnamAinda não há avaliações
- Diagnosis Treatment of Resistant HypertensionDocumento68 páginasDiagnosis Treatment of Resistant HypertensionJacob Alexander MarpaungAinda não há avaliações
- Lower Is Better - FinalDocumento91 páginasLower Is Better - FinalJamsidul Hassan RajibAinda não há avaliações
- Chapter 35 PDFDocumento4 páginasChapter 35 PDFHarsha Jeevan Kishore KaranamAinda não há avaliações
- Biomedik 3 Rational TherapyDocumento51 páginasBiomedik 3 Rational TherapyMarissaMatinahoruAinda não há avaliações
- Raas BlockadeDocumento77 páginasRaas BlockadeStella CooKeyAinda não há avaliações
- IsolatedSystolicHTN PaperDocumento9 páginasIsolatedSystolicHTN Paperstarskyhutch0000Ainda não há avaliações
- CPG Hypertension 2018 (Autosaved)Documento55 páginasCPG Hypertension 2018 (Autosaved)Navina PurushotmananAinda não há avaliações
- Virta HealthDocumento18 páginasVirta Healthismail100% (1)
- Treatment of Hypertension: Jai Radhakrishnan, M.D. Division of NephrologyDocumento34 páginasTreatment of Hypertension: Jai Radhakrishnan, M.D. Division of NephrologyAndika HAinda não há avaliações
- Cardiovascular Disease and Dyslipidemia: Beyond LDLDocumento10 páginasCardiovascular Disease and Dyslipidemia: Beyond LDLGuillen CelisAinda não há avaliações
- Lower Is Better - No Evidence For Treating To Spepecific Lipid Targets & Use of StatinsDocumento59 páginasLower Is Better - No Evidence For Treating To Spepecific Lipid Targets & Use of StatinsJamsidul Hassan RajibAinda não há avaliações
- Millllllaaa 123Documento11 páginasMillllllaaa 123200742 Elya AmaliaAinda não há avaliações
- Managing Hypertension Using Synergistic Dual Fixed Dose CombinationDocumento37 páginasManaging Hypertension Using Synergistic Dual Fixed Dose CombinationSherlyPosumahAinda não há avaliações
- Benenson 2019Documento7 páginasBenenson 20190128 Nurul Wahidah YasidAinda não há avaliações
- Calcium Channel Blockers in Antihypertensive Treatment The Role of LecardipineDocumento35 páginasCalcium Channel Blockers in Antihypertensive Treatment The Role of LecardipineAndi WirawanAinda não há avaliações
- ATC Criticas+apresentaçåo Cópia CópiaDocumento34 páginasATC Criticas+apresentaçåo Cópia Cópiajramires37566100% (3)
- Ginjal Dan Hipertensi-1Documento132 páginasGinjal Dan Hipertensi-1YERNITA AGUSTINAinda não há avaliações
- D. P. Laporta MD SMBD-JGH Dept of Adult Critical CareDocumento40 páginasD. P. Laporta MD SMBD-JGH Dept of Adult Critical CareMARTINAinda não há avaliações
- JNC VIII Hypertension SaudiDocumento47 páginasJNC VIII Hypertension SaudiDavid Chandra EriksonAinda não há avaliações
- 2.heart Rate - An Emerging Risk Factor in CVDDocumento49 páginas2.heart Rate - An Emerging Risk Factor in CVDAkhil SharmaAinda não há avaliações
- Guidelines Made Simple 2017 HBPDocumento28 páginasGuidelines Made Simple 2017 HBPThomas EipeAinda não há avaliações
- Management of Hypertension and Dyslipidemia in 2016 Daniel Tarditi, DODocumento27 páginasManagement of Hypertension and Dyslipidemia in 2016 Daniel Tarditi, DOSinta ChoiAinda não há avaliações
- Understanding The Needs of The High Productive DyslipidemiaDocumento47 páginasUnderstanding The Needs of The High Productive DyslipidemiachchchchkAinda não há avaliações
- Lipid Treatments in Cardiologic, Metabolic and Diabetics: From Guideline To Clinical PracticeDocumento65 páginasLipid Treatments in Cardiologic, Metabolic and Diabetics: From Guideline To Clinical PracticeRoby KieranAinda não há avaliações
- The Importance of Potential Statin in High Risk PatientDocumento56 páginasThe Importance of Potential Statin in High Risk PatientAidil Fittriani AyuAinda não há avaliações
- Guidline Peripheral Artery DiseaseDocumento104 páginasGuidline Peripheral Artery DiseaseAgung Anom Arie WiradanaAinda não há avaliações
- Prevention of Atherosclerotic Cardiovascular Disease - Guideline Updates On Blood Pressure and Cholesterol ControlDocumento64 páginasPrevention of Atherosclerotic Cardiovascular Disease - Guideline Updates On Blood Pressure and Cholesterol ControlNick NorgardAinda não há avaliações
- Hipertensiunea Arteriala - IiDocumento35 páginasHipertensiunea Arteriala - IiAndrei CiobotaruAinda não há avaliações
- Antagonis Reseptor Angiotensin 2, AIIRADocumento31 páginasAntagonis Reseptor Angiotensin 2, AIIRAsuho exoAinda não há avaliações
- Management of HPDocumento54 páginasManagement of HPDaud AbadiAinda não há avaliações
- Screenshot 2023-10-04 at 09.15.05Documento1 páginaScreenshot 2023-10-04 at 09.15.05Joe DrumAinda não há avaliações
- Hypertension Management: Is Beta Blockers Still EffectiveDocumento55 páginasHypertension Management: Is Beta Blockers Still EffectiveRidyahningtyas SintowatiAinda não há avaliações
- 080630 고혈압최신지견 (조장현 과장님)Documento46 páginas080630 고혈압최신지견 (조장현 과장님)hongmyongAinda não há avaliações
- Trends in Cardiovascular Medicine: John M. Flack, Bemi AdekolaDocumento5 páginasTrends in Cardiovascular Medicine: John M. Flack, Bemi Adekolaketut adiAinda não há avaliações
- Guidelines DyslipidDocumento49 páginasGuidelines Dyslipidnoveldycb89Ainda não há avaliações
- RidkerJUPITERslides - MPT - sld1Documento12 páginasRidkerJUPITERslides - MPT - sld1Nawel BenAinda não há avaliações
- HypertensionDocumento54 páginasHypertensionAli Murtaza AbbasAinda não há avaliações
- DR - Antonia Anna Lukito Slide - Webinar 18 April 2020Documento34 páginasDR - Antonia Anna Lukito Slide - Webinar 18 April 2020fairuzAinda não há avaliações
- Guias Hta 2022Documento8 páginasGuias Hta 2022oriannaocantoAinda não há avaliações
- Pitavastatin 4mgDocumento48 páginasPitavastatin 4mg松山內科部Ainda não há avaliações
- New Developments in The Management of DyslipidemiaDocumento63 páginasNew Developments in The Management of DyslipidemiaM Azmi HAinda não há avaliações
- Complete Blood Count (CBC With E.S.R) .: Investigation Units Result Biological Reference IntervalDocumento4 páginasComplete Blood Count (CBC With E.S.R) .: Investigation Units Result Biological Reference Intervalmaryam.ksohrabAinda não há avaliações
- Hipertension Arterial 2018Documento5 páginasHipertension Arterial 2018HIilda V. SerranoAinda não há avaliações
- Case-Based Panel Discussion NYHA II Post Hospitalization - Misperception of Risk - VF 1Documento47 páginasCase-Based Panel Discussion NYHA II Post Hospitalization - Misperception of Risk - VF 1VivekanandGuptaAinda não há avaliações
- Cholesterol Guidelines Review 2020Documento6 páginasCholesterol Guidelines Review 2020oriannaocantoAinda não há avaliações
- Hypertension General Overview GuidelinesDocumento62 páginasHypertension General Overview GuidelinesJuwanto WakiminAinda não há avaliações
- Diagnosis Dan Tatalaksana Hipertensi: Lab/Smf Ipd - Fkub-Rssa Malang 2018Documento52 páginasDiagnosis Dan Tatalaksana Hipertensi: Lab/Smf Ipd - Fkub-Rssa Malang 2018wahyu sandikaAinda não há avaliações
- CHADS2Documento1 páginaCHADS2Jose Villalobos PradoAinda não há avaliações
- Ambulatory Blood Pressure JournalDocumento7 páginasAmbulatory Blood Pressure JournalApt RiskaAinda não há avaliações
- CASE 1 GBS ADULT Patient Data BaseDocumento5 páginasCASE 1 GBS ADULT Patient Data Basequina mjAinda não há avaliações
- Blockade R A SDocumento20 páginasBlockade R A SAlaa KhazalehAinda não há avaliações
- Heart Rate Reduction in Heart Failure and Angina: A Paradox?Documento42 páginasHeart Rate Reduction in Heart Failure and Angina: A Paradox?Pratik SahaAinda não há avaliações
- Acid-Base Disorders: Clinical Evaluation and ManagementNo EverandAcid-Base Disorders: Clinical Evaluation and ManagementAinda não há avaliações
- Geriatri September Sampai Desember 2018Documento20 páginasGeriatri September Sampai Desember 2018Lia hermawatiAinda não há avaliações
- Pengaruh Kompres Hangat Jahe Merah (Zingiber Officinale Reumatoid Pada Lansia Di Upt. Pelayanan Sosial Lanjut Usia Dan Anak Balita Wilayah Binjai Dan Medan Sunarti AlhudaDocumento13 páginasPengaruh Kompres Hangat Jahe Merah (Zingiber Officinale Reumatoid Pada Lansia Di Upt. Pelayanan Sosial Lanjut Usia Dan Anak Balita Wilayah Binjai Dan Medan Sunarti AlhudaTaufikAinda não há avaliações
- Pengaruh Kompres Serei Hangat Terhadap Penurunan Intensitas Nyeri Artritis Rheumatoid Pada Lanjut UsiaDocumento16 páginasPengaruh Kompres Serei Hangat Terhadap Penurunan Intensitas Nyeri Artritis Rheumatoid Pada Lanjut UsiaLinda LidyanaAinda não há avaliações
- Jadwal Sympo Edit1Documento3 páginasJadwal Sympo Edit1reyAinda não há avaliações
- Acute Coronary Syndrome: Cardiology Bethesda Hospital Yogyakarta Dr. Lidwina Tarigan SPJPDocumento40 páginasAcute Coronary Syndrome: Cardiology Bethesda Hospital Yogyakarta Dr. Lidwina Tarigan SPJPPalupiPuspitoRiniAinda não há avaliações
- Nama: Bilqis Inas Nur Hanifah NIM: 021411131041 Obat - Obat Beta BlockersDocumento3 páginasNama: Bilqis Inas Nur Hanifah NIM: 021411131041 Obat - Obat Beta BlockersbilqisinasAinda não há avaliações
- Hypertension and Cognitive ImpairmentDocumento3 páginasHypertension and Cognitive ImpairmentMekonninAinda não há avaliações
- Isilimela Hospital Speech Therapy DepartmentDocumento2 páginasIsilimela Hospital Speech Therapy DepartmentSuné GreeffAinda não há avaliações
- Laporan Pasien Konsul Divisi Endokrin FauzanDocumento2 páginasLaporan Pasien Konsul Divisi Endokrin Fauzanfauzan azhariAinda não há avaliações
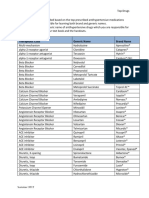
- Top Antihypertensive Drugs Generic-Brand Names PDFDocumento1 páginaTop Antihypertensive Drugs Generic-Brand Names PDFvidbala0% (1)
- How Alois Alzheimer Redefined DementiaDocumento4 páginasHow Alois Alzheimer Redefined DementiaElaineWilliamsAinda não há avaliações
- Perbandingan Siriraj Skor (SS) Dan Algoritma Gajah Mada (Agm) Kasus Stroke Di Igd Rsud Dr. Soedono MadiunDocumento5 páginasPerbandingan Siriraj Skor (SS) Dan Algoritma Gajah Mada (Agm) Kasus Stroke Di Igd Rsud Dr. Soedono MadiunMutiara FadilahAinda não há avaliações
- 579-Article Text-1710-1-10-20220113Documento10 páginas579-Article Text-1710-1-10-20220113Nurul AdibahAinda não há avaliações
- Stroke Teaching Course: Brasov, Romania January 25-27, 2024Documento4 páginasStroke Teaching Course: Brasov, Romania January 25-27, 2024Catalina NastasaAinda não há avaliações
- Easy Hypertension ClassificationDocumento1 páginaEasy Hypertension ClassificationGirish WaruAinda não há avaliações
- Daftar Pustaka StrokeDocumento5 páginasDaftar Pustaka StrokeWilliam WiryawanAinda não há avaliações
- ARC Library On Alzheimer's DiseaseDocumento10 páginasARC Library On Alzheimer's Diseaserbs6610100% (1)
- Bi-Preterax Slide Set CI 15 - 16Documento35 páginasBi-Preterax Slide Set CI 15 - 16drnasim20088171Ainda não há avaliações
- Sistem Pakar Diagnosa Kelainan Sistem Ortopedi Pada Manusia Dengan Metode Forward Chaining Dan Dempster ShaferDocumento10 páginasSistem Pakar Diagnosa Kelainan Sistem Ortopedi Pada Manusia Dengan Metode Forward Chaining Dan Dempster Shafernurhaini rahmawatiAinda não há avaliações
- Hipertensi JNC 1-8Documento1 páginaHipertensi JNC 1-8Windyanissa RecitaAinda não há avaliações
- Hypertensive Emgerencies 2021Documento19 páginasHypertensive Emgerencies 2021Faranitach AiniAinda não há avaliações
- Daftar Judul Poster AOCN PembimbingDocumento3 páginasDaftar Judul Poster AOCN PembimbingWaskitho NugrohoAinda não há avaliações
- Hubungan Pengetahuan Dan Sikap Dengan Peran Perawat Pasca Pemberian Terapi RtpaDocumento6 páginasHubungan Pengetahuan Dan Sikap Dengan Peran Perawat Pasca Pemberian Terapi RtpafatmawatiAinda não há avaliações
- Ikfr - MM Sken 3Documento3 páginasIkfr - MM Sken 36130017050 RISMA MIFTAHUL JANNAHAinda não há avaliações
- Pengaruh Range of Motion (Rom) Aktif Dan Pasif Terhadap Rentang Gerak Pada Lansia Yang Mengalami Artitis Rematoid Di Kota BengkuluDocumento11 páginasPengaruh Range of Motion (Rom) Aktif Dan Pasif Terhadap Rentang Gerak Pada Lansia Yang Mengalami Artitis Rematoid Di Kota BengkuluNanda MaisyuriAinda não há avaliações
- MINDMAPDocumento2 páginasMINDMAPrayzaoliveira.ausAinda não há avaliações
- 199-Article Text-1111-1-10-20230613Documento7 páginas199-Article Text-1111-1-10-20230613Yayu AngrianAinda não há avaliações
- Analisa Jurnal: Evidence Based Practice (Ebp)Documento9 páginasAnalisa Jurnal: Evidence Based Practice (Ebp)Arum pawestriAinda não há avaliações
- Faktor PICODocumento1 páginaFaktor PICOAlldo SaodalaAinda não há avaliações
- AlzheimersDocumento25 páginasAlzheimersSafrizalAinda não há avaliações