Você também pode gostar
- ECGDocumento41 páginasECGmiguel mendezAinda não há avaliações
- All EcgDocumento143 páginasAll EcgYenza FaheraAinda não há avaliações
- Basic ECG ReadingDocumento41 páginasBasic ECG ReadingBenj100% (4)
- Uworld Step 2 CK Charts-OcrDocumento440 páginasUworld Step 2 CK Charts-OcrIvory Jameston100% (2)
- ECG WorldDocumento139 páginasECG WorldsatyaAinda não há avaliações
- Normal ECGDocumento63 páginasNormal ECGMohd Johari Mohd ShafuwanAinda não há avaliações
- Simple Guide To Ecg InterpretationDocumento53 páginasSimple Guide To Ecg Interpretationedy suyantoAinda não há avaliações
- Ekg Normal Dan Acs Sudin TimurDocumento59 páginasEkg Normal Dan Acs Sudin TimurArum MaharaniAinda não há avaliações
- ECG Normal and AbnormalDocumento74 páginasECG Normal and Abnormalawaniedream8391100% (1)
- Basic ECG InterpretationDocumento61 páginasBasic ECG InterpretationIndra ChristiantoAinda não há avaliações
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookAinda não há avaliações
- Kuliah Ekg UnswagatiDocumento75 páginasKuliah Ekg UnswagatiiikAinda não há avaliações
- Dr. Adeel Ahmed Waheed: House Officer M-4Documento84 páginasDr. Adeel Ahmed Waheed: House Officer M-4Hussain AzharAinda não há avaliações
- Basics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyDocumento206 páginasBasics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyRavi SharmaAinda não há avaliações
- ELECTROCARDIOGRAPHYDocumento75 páginasELECTROCARDIOGRAPHYMeliaAinda não há avaliações
- ElectrocardiogramDocumento169 páginasElectrocardiogramjitendra magarAinda não há avaliações
- Ecg Made EasyDocumento130 páginasEcg Made EasyJOHN ARBIE TATTAO, RN96% (49)
- Equine Dorsoscapular LigamentDocumento7 páginasEquine Dorsoscapular Ligamentcharlie100% (1)
- Didactics ECGDocumento87 páginasDidactics ECGGenesis Poblacion100% (1)
- Electrocardiography: I. Leads A. Limb LeadsDocumento11 páginasElectrocardiography: I. Leads A. Limb LeadsJoezelle0% (1)
- Asist. Univ. Dr. Mihaela Popescu Catedra de Cardiologie Spitalul Universitar de Urgenta EliasDocumento64 páginasAsist. Univ. Dr. Mihaela Popescu Catedra de Cardiologie Spitalul Universitar de Urgenta EliasAnonymous CQmrhq1O7Ainda não há avaliações
- Basic Ecg: - Department of Medicine BIMC Hospital 2013Documento60 páginasBasic Ecg: - Department of Medicine BIMC Hospital 2013LexadkAinda não há avaliações
- Basic ECG Interpretation: Cardiology and Vascular Department Medical Faculty of Hasanuddin UniversityDocumento61 páginasBasic ECG Interpretation: Cardiology and Vascular Department Medical Faculty of Hasanuddin UniversityHayat Hamzah DawiAinda não há avaliações
- Facial Danger ZonesDocumento29 páginasFacial Danger ZonesShamad AbduAinda não há avaliações
- Pathophysiology Total Anterior Circulation Infarction Left Middle Cerebral Artery (TACILMCA)Documento2 páginasPathophysiology Total Anterior Circulation Infarction Left Middle Cerebral Artery (TACILMCA)PATHOSHOPPE100% (1)
- Basic of EcgDocumento82 páginasBasic of Ecgpopescuioana1Ainda não há avaliações
- Materi Dasar EkgDocumento52 páginasMateri Dasar EkgFirsandiPrasastyaFikryGozali100% (2)
- ECG Normal - ErwanDocumento49 páginasECG Normal - ErwanEvelyne NatalieAinda não há avaliações
- Interpretasi Elektrokardiografi: Dr. Erlina Marfianti, MSC, SPPD Departemen Ilmu Penyakit Dalam Fakultas Kedokteran UiiDocumento60 páginasInterpretasi Elektrokardiografi: Dr. Erlina Marfianti, MSC, SPPD Departemen Ilmu Penyakit Dalam Fakultas Kedokteran UiiArif Zulfian MubarokAinda não há avaliações
- Normal Electrocardiogram: Lucia Kris Dinarti Cardiology Department Faculty of Medicine GMUDocumento21 páginasNormal Electrocardiogram: Lucia Kris Dinarti Cardiology Department Faculty of Medicine GMUMuhammad Ricky RamadhianAinda não há avaliações
- Interpretasi ElektrokardiografiDocumento60 páginasInterpretasi ElektrokardiografiYogi GustriansyahAinda não há avaliações
- DASAR KURSUS EKG - DR WiryawanDocumento68 páginasDASAR KURSUS EKG - DR WiryawanElsa TjahyaAinda não há avaliações
- Ecg Presentation 2013Documento40 páginasEcg Presentation 2013Samuel FpAinda não há avaliações
- The Normal ElectrocardiogramDocumento63 páginasThe Normal ElectrocardiogramPuravin Crishan VeerasamyAinda não há avaliações
- Department of Cardiology and Vascular Medicine, Padjadjaran University School of Medicine Hasan Sadikin Hospital BandungDocumento61 páginasDepartment of Cardiology and Vascular Medicine, Padjadjaran University School of Medicine Hasan Sadikin Hospital BandungMuhammad AmrieAinda não há avaliações
- THE Electrocardiogram (Ecg / Ekg) : By: DR Yasir MansouriDocumento83 páginasTHE Electrocardiogram (Ecg / Ekg) : By: DR Yasir Mansourirofi modiAinda não há avaliações
- Basics of ElectrocardiographyDocumento227 páginasBasics of ElectrocardiographyVlad CarabinAinda não há avaliações
- Interpretasi ElektrokardiografiDocumento60 páginasInterpretasi ElektrokardiografiAditya Praja'schAinda não há avaliações
- Dasar-Dasar Interpretasi EKGDocumento61 páginasDasar-Dasar Interpretasi EKGFatmawati nersAinda não há avaliações
- Basics of Ecg: DR Shyama Assistant Professor General Medicine Aiims, PatnaDocumento117 páginasBasics of Ecg: DR Shyama Assistant Professor General Medicine Aiims, PatnaSimran KothariAinda não há avaliações
- 07.01 - 12 Lead ECG Interpretation 2019Documento141 páginas07.01 - 12 Lead ECG Interpretation 2019Lana LocoAinda não há avaliações
- Cardio INTERPRETATION OF THE ELECTROCARDIOGRAMDocumento74 páginasCardio INTERPRETATION OF THE ELECTROCARDIOGRAMkrisnoAinda não há avaliações
- Electrocardiogram (ECG) : This Is The Lecture No. 4Documento51 páginasElectrocardiogram (ECG) : This Is The Lecture No. 4Aboodsha ShAinda não há avaliações
- EcgDocumento6 páginasEcgMohamed IbrahimAinda não há avaliações
- Basics of ECG Pre-Workshop: Dr. Nancy Selfridge Chair, Department of Clinical Medicine Semester 4 2019Documento43 páginasBasics of ECG Pre-Workshop: Dr. Nancy Selfridge Chair, Department of Clinical Medicine Semester 4 2019Tom TsouAinda não há avaliações
- The Normal Adult ECGDocumento84 páginasThe Normal Adult ECGkimiastroAinda não há avaliações
- Interpretasi ElektrokardiogramDocumento36 páginasInterpretasi ElektrokardiogramendahAinda não há avaliações
- Anatomi 1Documento54 páginasAnatomi 1Fany LainamaAinda não há avaliações
- Matrikulasi Interpretasi EkgDocumento40 páginasMatrikulasi Interpretasi Ekgsupergirl2123Ainda não há avaliações
- KULIAH ECG Dinkes PurworejoDocumento69 páginasKULIAH ECG Dinkes PurworejoVella NurfatimahAinda não há avaliações
- Elektrokardiografi Dasar: Dr. Eka Ginanjar, SPPDDocumento81 páginasElektrokardiografi Dasar: Dr. Eka Ginanjar, SPPDNur Rahmat WibowoAinda não há avaliações
- KULIAH ECG Dinkes PurworejoDocumento69 páginasKULIAH ECG Dinkes PurworejoSofian PalupiAinda não há avaliações
- Ecg Basics - NAVEENDocumento65 páginasEcg Basics - NAVEENNaveen MathieuAinda não há avaliações
- Dasar-Dasar EkgDocumento67 páginasDasar-Dasar EkgIGD Kenak MedikaAinda não há avaliações
- ECG Reading: The Common and DangerousDocumento77 páginasECG Reading: The Common and DangerousFitri UlansariAinda não há avaliações
- Ecg Interpretation:: The BasicsDocumento40 páginasEcg Interpretation:: The BasicsRavi SharmaAinda não há avaliações
- Pemasangan Dan Interpretasi EKGDocumento117 páginasPemasangan Dan Interpretasi EKGaulianadanisya100% (2)
- Normal Sinus RhythmDocumento48 páginasNormal Sinus RhythmStella mAinda não há avaliações
- Dasar Kursus EKG - DR ParwataDocumento67 páginasDasar Kursus EKG - DR ParwataPuka Putra AdnyanaAinda não há avaliações
- Understanding Intracardiac EGMs: A Patient Centered GuideNo EverandUnderstanding Intracardiac EGMs: A Patient Centered GuideAinda não há avaliações
- BIRADSDocumento94 páginasBIRADSSergio MoralesAinda não há avaliações
- Book Reviews: Contemporary Oral and Maxillofacial Surgery, 6Th EditionDocumento1 páginaBook Reviews: Contemporary Oral and Maxillofacial Surgery, 6Th EditionPark SuriAinda não há avaliações
- Varicose Veins Treatment by VSLSDocumento10 páginasVaricose Veins Treatment by VSLSravuljindalAinda não há avaliações
- Anesthetic Management and Deep Sedation After Emergence From General Anesthesia - A Retrospective Cohort StudyDocumento10 páginasAnesthetic Management and Deep Sedation After Emergence From General Anesthesia - A Retrospective Cohort Studygwhqvmqks5Ainda não há avaliações
- Annotated Bibliography 1Documento2 páginasAnnotated Bibliography 1api-663775614Ainda não há avaliações
- When To Stop CPRDocumento32 páginasWhen To Stop CPRpdccAinda não há avaliações
- Congenital Anomalies and Variations of The Bile and Pancreatic Ducts - Magnetic Resonance Cholangiopancreatography Findings, Epidemiology and Clinical SignificanceDocumento19 páginasCongenital Anomalies and Variations of The Bile and Pancreatic Ducts - Magnetic Resonance Cholangiopancreatography Findings, Epidemiology and Clinical SignificanceRoberto HernandezAinda não há avaliações
- Macro PneumohemoDocumento28 páginasMacro PneumohemoSiti AishahAinda não há avaliações
- Apfs 2012 MidDocumento79 páginasApfs 2012 Middaniel meresaAinda não há avaliações
- Malay, Age: 59 Years Old, Date of Admission: 18 August 2009 (CCU), 26 August 2009 (Ward 6B), Date of Clerking: 26 August 2009, Source ofDocumento8 páginasMalay, Age: 59 Years Old, Date of Admission: 18 August 2009 (CCU), 26 August 2009 (Ward 6B), Date of Clerking: 26 August 2009, Source ofAiman ArifinAinda não há avaliações
- Tracheostomy CareDocumento7 páginasTracheostomy CareICNREVILOAinda não há avaliações
- Ileo Biliar Inukai 2019Documento4 páginasIleo Biliar Inukai 2019stefanyAinda não há avaliações
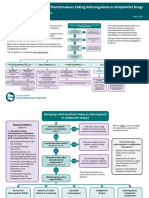
- Sdcep Anticoagulants Quick Reference Guide 2nd EditionDocumento5 páginasSdcep Anticoagulants Quick Reference Guide 2nd EditionMeryem LahlouAinda não há avaliações
- Stainless Steel CrownsDocumento19 páginasStainless Steel CrownsSameerChoudharyAinda não há avaliações
- Tecres, Bone Cement, Tecres CemexDocumento12 páginasTecres, Bone Cement, Tecres CemexMahsaAinda não há avaliações
- ENT Batch 2022 Annual Paper-1Documento9 páginasENT Batch 2022 Annual Paper-1mudassirahmedAinda não há avaliações
- Abdomen CAP Questions and AnswersDocumento6 páginasAbdomen CAP Questions and AnswersRathnaAinda não há avaliações
- Echocardiographic Evaluation of Patent Foramen Ovale Prior To Device ClosureDocumento12 páginasEchocardiographic Evaluation of Patent Foramen Ovale Prior To Device ClosureIris AszalosAinda não há avaliações
- 2-NPSG Chapter OBS Jan2023Documento8 páginas2-NPSG Chapter OBS Jan2023Blanca LanderosAinda não há avaliações
- Journal of Pediatric Surgery: Ibrahim UygunDocumento4 páginasJournal of Pediatric Surgery: Ibrahim UygunNur Ainatun NadrahAinda não há avaliações
- Introduction To NeuroanatomyDocumento20 páginasIntroduction To NeuroanatomySurjagnee SannyamatAinda não há avaliações
- 4.the Management of Patients On Anticoagulants Prior.16Documento8 páginas4.the Management of Patients On Anticoagulants Prior.16Gabriela Catana TurcuAinda não há avaliações
- Induction of Labor Algorithm: Appendix RDocumento1 páginaInduction of Labor Algorithm: Appendix RBrolie BarsebaAinda não há avaliações
- HaseebaK EtalDocumento5 páginasHaseebaK EtalIndah VitasariAinda não há avaliações
- Tympanoplasty Excellent Summary1Documento29 páginasTympanoplasty Excellent Summary1DrMohmd ZidaanAinda não há avaliações
- 1843 FullDocumento123 páginas1843 FullKevin KnightsAinda não há avaliações