Você também pode gostar
- Sample Death CertificateDocumento4 páginasSample Death Certificatenashobo67% (3)
- Death Certificate of My Dad's Protege, Edward A. Patrick MD PHD, Ohio Department of Health, 12/23/09Documento1 páginaDeath Certificate of My Dad's Protege, Edward A. Patrick MD PHD, Ohio Department of Health, 12/23/09Peter M. HeimlichAinda não há avaliações
- Laurel SFDocumento3 páginasLaurel SFEllyn SantiagoAinda não há avaliações
- PghyfhbDocumento2 páginasPghyfhbapi-356485954Ainda não há avaliações
- Commonwealth of Kentucky Proof of Insurance: Insurance Company Agency/Company Issuing Card Our Contact InformationDocumento3 páginasCommonwealth of Kentucky Proof of Insurance: Insurance Company Agency/Company Issuing Card Our Contact InformationRobert TaylorAinda não há avaliações
- Policy Vaccination Record CardDocumento2 páginasPolicy Vaccination Record CardGurpreetAinda não há avaliações
- Member Data Record: Philippine Health Insurance CorporationDocumento1 páginaMember Data Record: Philippine Health Insurance CorporationKristine OgalescoAinda não há avaliações
- MBPD Report 19023065 - Assault - 10-12Documento3 páginasMBPD Report 19023065 - Assault - 10-12ABC15 NewsAinda não há avaliações
- Cody Tuomala Death CertificationDocumento1 páginaCody Tuomala Death CertificationJeff TuomalaAinda não há avaliações
- Official MDR PDFDocumento1 páginaOfficial MDR PDFBesarioLouiseCassandraAinda não há avaliações
- Covid-19 Test Result Summary: Sars-Cov-2 Viral Rna - Not DetectedDocumento1 páginaCovid-19 Test Result Summary: Sars-Cov-2 Viral Rna - Not DetectedRodel OrtegaAinda não há avaliações
- MPD Police ReportDocumento3 páginasMPD Police ReportWJLA-TVAinda não há avaliações
- Seattle Police Report During BLM RiotDocumento5 páginasSeattle Police Report During BLM RiotDebra KolrudAinda não há avaliações
- Miami Beach Police Jonathan Alonso Arrest FormDocumento2 páginasMiami Beach Police Jonathan Alonso Arrest FormRandom Pixels blogAinda não há avaliações
- Employment Application Template 25Documento6 páginasEmployment Application Template 25Romee SinghAinda não há avaliações
- Stauch USAADocumento47 páginasStauch USAALeigh EganAinda não há avaliações
- SMUKVAFDocumento8 páginasSMUKVAFAnonymous 8gF1ZI4SVMAinda não há avaliações
- ASSE - World Heritage ID CardDocumento1 páginaASSE - World Heritage ID CardNishat T TiothyAinda não há avaliações
- Event 18174187 Public Incident PacketDocumento1 páginaEvent 18174187 Public Incident PacketWJLA-TVAinda não há avaliações
- Fulton County Police ReportDocumento4 páginasFulton County Police ReportJulie Wolfe100% (1)
- Denton Police Supplement ReportDocumento2 páginasDenton Police Supplement Reportwfaachannel8Ainda não há avaliações
- Abu Dhabi Police GHQ - E-Services - Payment ReceiptDocumento1 páginaAbu Dhabi Police GHQ - E-Services - Payment Receiptgk100% (1)
- Barrington Residential Prospective Resident Application ProcessDocumento5 páginasBarrington Residential Prospective Resident Application Process568224736Ainda não há avaliações
- GeicoDocumento2 páginasGeicotfuyuicgufgyu5469Ainda não há avaliações
- Aaron Kali Quinones Arrested and Charged With Attempted Felony Murder in Miami-Dade County, FL - Jan. 2, 2022Documento2 páginasAaron Kali Quinones Arrested and Charged With Attempted Felony Murder in Miami-Dade County, FL - Jan. 2, 2022Omar Rodriguez OrtizAinda não há avaliações
- Lab ReportDocumento1 páginaLab ReportNishantAinda não há avaliações
- Sentencing Memorandum For Amit PatelDocumento67 páginasSentencing Memorandum For Amit PatelActionNewsJaxAinda não há avaliações
- David Archie DivorceDocumento9 páginasDavid Archie Divorcethe kingfishAinda não há avaliações
- San Diego County Birth Certificate ApplicationDocumento2 páginasSan Diego County Birth Certificate ApplicationFootballBeastAinda não há avaliações
- Inman ComplaintDocumento13 páginasInman ComplaintJessica Madeline PaskoAinda não há avaliações
- I 485 Cabrera Alonso, MeidelynDocumento18 páginasI 485 Cabrera Alonso, MeidelynMeidelyn CabreraAinda não há avaliações
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Section A - Patient DetailsDocumento2 páginasIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Section A - Patient DetailsPcrAinda não há avaliações
- Rellance: Laikshmlovaa PDST, Dasanaputa Holl Tanna LnreDocumento16 páginasRellance: Laikshmlovaa PDST, Dasanaputa Holl Tanna LnreSanthosh RAinda não há avaliações
- MCSO 19OFF028747 Incident Report Tag StolenDocumento8 páginasMCSO 19OFF028747 Incident Report Tag StolenNeil GillespieAinda não há avaliações
- 2013 Groping and Indecent ExposureDocumento4 páginas2013 Groping and Indecent ExposureDanielle SalisburyAinda não há avaliações
- Change of Landlord Agent FormDocumento2 páginasChange of Landlord Agent FormimiescribdAinda não há avaliações
- Asylum SeekerDocumento3 páginasAsylum SeekerAdv Mahmudur RashidAinda não há avaliações
- Vehicle Insurance Certificate PDF Template PDFDocumento1 páginaVehicle Insurance Certificate PDF Template PDFstudent sAinda não há avaliações
- Id Cards American Alliance 34567890Documento1 páginaId Cards American Alliance 34567890xxoreocandyyxxAinda não há avaliações
- Incident Report of Miami-Dade Police Officer Donovan William Rojas - June 12, 202Documento14 páginasIncident Report of Miami-Dade Police Officer Donovan William Rojas - June 12, 202Omar Rodriguez Ortiz100% (1)
- Burr Ridge Police Report Devette CobbsDocumento9 páginasBurr Ridge Police Report Devette CobbsDavid GiulianiAinda não há avaliações
- INSURENCE TerryDocumento1 páginaINSURENCE TerryRaymi TejadaAinda não há avaliações
- Death Certificate NagendraDocumento1 páginaDeath Certificate NagendraYannam Siva nagendraAinda não há avaliações
- Test ResultDocumento1 páginaTest ResultSofia100% (1)
- Formsoppsapplication Illinois Birth Record 2018Documento2 páginasFormsoppsapplication Illinois Birth Record 2018CynthiaAinda não há avaliações
- Police Clearance: National Police Commission Philippine National PoliceDocumento1 páginaPolice Clearance: National Police Commission Philippine National PolicecperaltavelascoAinda não há avaliações
- DeathCertificate PDFDocumento3 páginasDeathCertificate PDFUrischarAinda não há avaliações
- PHN SAMPLE AppDocumento3 páginasPHN SAMPLE AppRosemaryCastroAinda não há avaliações
- Generate Certificate 1628006671176Documento1 páginaGenerate Certificate 1628006671176Ahsan Sajjad100% (1)
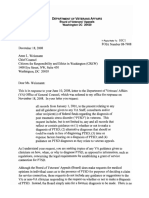
- CREW: Department of Veterans Affairs: Regarding PTSD Diagnosis: Cover Letter 121808Documento2 páginasCREW: Department of Veterans Affairs: Regarding PTSD Diagnosis: Cover Letter 121808CREWAinda não há avaliações
- Gloria JamesDocumento4 páginasGloria JamesUSA TODAYAinda não há avaliações
- MS Birth Cert. AppDocumento2 páginasMS Birth Cert. AppJonathanKiehlAinda não há avaliações
- Health Insurance Spring 2017Documento2 páginasHealth Insurance Spring 2017Manideep RemalaAinda não há avaliações
- 4600229175 - CopyDocumento2 páginas4600229175 - CopyData BaseAinda não há avaliações
- Complete Report OAPR-77102 Praveen 29aug2019Documento13 páginasComplete Report OAPR-77102 Praveen 29aug2019Praveen MNAinda não há avaliações
- Saro ComplaintDocumento6 páginasSaro ComplaintBayAreaNewsGroupAinda não há avaliações
- California Insurance ID Card Effective DDocumento1 páginaCalifornia Insurance ID Card Effective DD BAinda não há avaliações
- Divorce CertificateDocumento1 páginaDivorce Certificatestulio7Ainda não há avaliações
- Certificate of Death (Municipal Form 103)Documento2 páginasCertificate of Death (Municipal Form 103)Carmi Anne Jurado DomingoAinda não há avaliações
- Certificate of DeathDocumento2 páginasCertificate of DeathBeyza Gemici0% (1)
- Fash Mags Advt ContactsDocumento2 páginasFash Mags Advt ContactsMamillapalli ChowdaryAinda não há avaliações
- Interior SyllabusDocumento3 páginasInterior SyllabusMamillapalli ChowdaryAinda não há avaliações
- Career Options After Fashion DesignDocumento3 páginasCareer Options After Fashion DesignMamillapalli ChowdaryAinda não há avaliações
- BAZAAR - 2019 - Advertising RatesDocumento1 páginaBAZAAR - 2019 - Advertising RatesMamillapalli ChowdaryAinda não há avaliações
- Fashion SyllabusDocumento2 páginasFashion SyllabusMamillapalli ChowdaryAinda não há avaliações
- Nata CentersDocumento3 páginasNata CentersMamillapalli ChowdaryAinda não há avaliações
- Career Options PresentationDocumento3 páginasCareer Options PresentationMamillapalli ChowdaryAinda não há avaliações
- 10 Career Options After Becoming An Interior DesignerDocumento3 páginas10 Career Options After Becoming An Interior DesignerMamillapalli ChowdaryAinda não há avaliações
- Career Test ProposalDocumento2 páginasCareer Test ProposalMamillapalli ChowdaryAinda não há avaliações
- Black Orange and Yellow Simple PMI Charts Poster PDFDocumento1 páginaBlack Orange and Yellow Simple PMI Charts Poster PDFMamillapalli ChowdaryAinda não há avaliações
- Career Guide - High SchoolDocumento119 páginasCareer Guide - High SchoolHersey Badulis HernandezAinda não há avaliações
- Career Test ProposalDocumento2 páginasCareer Test ProposalMamillapalli ChowdaryAinda não há avaliações
- All The BestDocumento1 páginaAll The BestMamillapalli ChowdaryAinda não há avaliações
- JD FaqDocumento1 páginaJD FaqMamillapalli ChowdaryAinda não há avaliações
- Affiliation Completed CollegesDocumento4 páginasAffiliation Completed CollegesMamillapalli ChowdaryAinda não há avaliações
- Social Media Marketing PDFDocumento34 páginasSocial Media Marketing PDFMamillapalli ChowdaryAinda não há avaliações
- Careerinfashiondesigning 160304043541Documento30 páginasCareerinfashiondesigning 160304043541Mamillapalli ChowdaryAinda não há avaliações
- ACCA-CIMA March19Documento4 páginasACCA-CIMA March19Mamillapalli ChowdaryAinda não há avaliações
- Affiliation Completed CollegesDocumento7 páginasAffiliation Completed CollegesMamillapalli ChowdaryAinda não há avaliações
- Fashion Designer FAQDocumento7 páginasFashion Designer FAQMamillapalli ChowdaryAinda não há avaliações
- Syllabus - All COURSES & SemestersDocumento15 páginasSyllabus - All COURSES & SemestersMamillapalli ChowdaryAinda não há avaliações
- Affiliation Completed CollegesDocumento7 páginasAffiliation Completed CollegesMamillapalli ChowdaryAinda não há avaliações
- 2 Feedback FormDocumento1 página2 Feedback FormMamillapalli ChowdaryAinda não há avaliações
- Affiliation Completed CollegesDocumento4 páginasAffiliation Completed CollegesMamillapalli ChowdaryAinda não há avaliações
- Death Certificate Template 14 PDFDocumento1 páginaDeath Certificate Template 14 PDFMamillapalli ChowdaryAinda não há avaliações
- Death Certificate Template 17Documento1 páginaDeath Certificate Template 17Mamillapalli ChowdaryAinda não há avaliações
- 31st AugustDocumento1 página31st AugustMamillapalli ChowdaryAinda não há avaliações
- Report Card Template 16.Documento6 páginasReport Card Template 16.Mamillapalli ChowdaryAinda não há avaliações
- Dermatology ResearchDocumento9 páginasDermatology ResearchjumaracruzAinda não há avaliações
- Podj 4 PDFDocumento3 páginasPodj 4 PDFNur Sita DewiAinda não há avaliações
- Avoiding The Internal Mammary Artery During Parasternal Blocks: Ultrasound Identification and Technique ConsiderationsDocumento9 páginasAvoiding The Internal Mammary Artery During Parasternal Blocks: Ultrasound Identification and Technique ConsiderationsTheUdoAinda não há avaliações
- Quick Guide To ProscriptDocumento20 páginasQuick Guide To ProscriptAmit Raj100% (2)
- Food Eponyms in Pathology PDFDocumento6 páginasFood Eponyms in Pathology PDFJose PhilipeAinda não há avaliações
- Presentasi Bio-Strath 2016Documento28 páginasPresentasi Bio-Strath 2016Imanluves Amel100% (1)
- Pediatric Voice PresentationDocumento16 páginasPediatric Voice Presentationapi-254429093Ainda não há avaliações
- Medications For Primary ComplexDocumento8 páginasMedications For Primary ComplexMary CruzAinda não há avaliações
- 2011 Pediatric Anesthesia - BissonnetteDocumento2.287 páginas2011 Pediatric Anesthesia - BissonnettePaulo HibernonAinda não há avaliações
- Foundations of Respiratory Medicine (2018) PDFDocumento375 páginasFoundations of Respiratory Medicine (2018) PDFCristinaLucanAinda não há avaliações
- Easy Health Insurance Claim FormDocumento3 páginasEasy Health Insurance Claim FormJanmejay SinghAinda não há avaliações
- MCAT SecretsDocumento32 páginasMCAT SecretsTunde Ipaye100% (2)
- Sun Salutations Yoga Lesson PlanDocumento8 páginasSun Salutations Yoga Lesson PlanErica Harris100% (1)
- Crossmatching, Types, Principle, Procedure and InterpretationDocumento5 páginasCrossmatching, Types, Principle, Procedure and InterpretationMerhan FoudaAinda não há avaliações
- IvabradineDocumento30 páginasIvabradinepashaAinda não há avaliações
- Munro 2007Documento17 páginasMunro 2007Jose RodriguezAinda não há avaliações
- Legal Aspects in NursingDocumento4 páginasLegal Aspects in Nursinghnybnch100% (1)
- Food Safety and StandardsDocumento8 páginasFood Safety and StandardsArifSheriffAinda não há avaliações
- Part B-25-Myths About Dental Care - Q&ADocumento5 páginasPart B-25-Myths About Dental Care - Q&Afernanda1rondelliAinda não há avaliações
- 2010 Article 319 PDFDocumento12 páginas2010 Article 319 PDFabarmasAinda não há avaliações
- 302333KW PDFDocumento19 páginas302333KW PDFdhineshAinda não há avaliações
- Tugas MedicineDocumento2 páginasTugas MedicineRiza Ikhsan MuliaAinda não há avaliações
- Classical Homoeopathy Book FourDocumento99 páginasClassical Homoeopathy Book FourYaniv Algrably100% (1)
- Compliance Program Guidance Manual 7341.002 PDFDocumento45 páginasCompliance Program Guidance Manual 7341.002 PDFpopatlilo2Ainda não há avaliações
- Laporan Kematian Pang Kim ChoonDocumento17 páginasLaporan Kematian Pang Kim ChoonAfifah SelamatAinda não há avaliações
- Premature Rupture of MembranesDocumento38 páginasPremature Rupture of MembranesArwa QishtaAinda não há avaliações
- Clinical Criteria For The Determination of Death: WHO Technical Expert ConsultationDocumento16 páginasClinical Criteria For The Determination of Death: WHO Technical Expert ConsultationNicholas TagleAinda não há avaliações
- Henoch Schonlein PurpuraDocumento28 páginasHenoch Schonlein PurpuraPhil Adit R100% (1)
- HAND HYGIENE MONITORING SHEET (Revised)Documento3 páginasHAND HYGIENE MONITORING SHEET (Revised)lance tabinasAinda não há avaliações
- Nursing Board Exam ReviewerDocumento32 páginasNursing Board Exam ReviewerRose Anne Mückl100% (9)