Você também pode gostar
- Aaendo Q&ADocumento50 páginasAaendo Q&Aanadelavega96Ainda não há avaliações
- Interceptive Orthodontics ReviewDocumento4 páginasInterceptive Orthodontics ReviewAyu Nur A'IniAinda não há avaliações
- Access Cavity Preparation FinalDocumento63 páginasAccess Cavity Preparation Finalrasagna reddyAinda não há avaliações
- A Pico EctomyDocumento74 páginasA Pico EctomyFatima SiddiquiAinda não há avaliações
- Immediate DenturesDocumento35 páginasImmediate DenturesSimran SahniAinda não há avaliações
- PMDC Inspection For CollegeDocumento16 páginasPMDC Inspection For CollegeAsif Manzoor100% (3)
- Starting A New Dental Practice Checklist PDFDocumento4 páginasStarting A New Dental Practice Checklist PDFAbdelrahman GalalAinda não há avaliações
- Basic Concepts of OcclusionDocumento107 páginasBasic Concepts of Occlusionaparna mohananithaAinda não há avaliações
- Gag Reflex ControlDocumento5 páginasGag Reflex ControlSalma RafiqAinda não há avaliações
- Prepro SurgeryDocumento155 páginasPrepro SurgeryNagham AhmedAinda não há avaliações
- Diagnosis and Treatment Planning For Partially Edentulous Patients11Documento160 páginasDiagnosis and Treatment Planning For Partially Edentulous Patients11Rajsandeep Singh80% (5)
- Cracked Tooth PresentationDocumento36 páginasCracked Tooth Presentationmirfanulhaq100% (1)
- Cochlear Implant Surgery Treatment & Management - Medical Therapy, Surgical Therapy, Preoperative DetailsDocumento9 páginasCochlear Implant Surgery Treatment & Management - Medical Therapy, Surgical Therapy, Preoperative DetailsFityah UfiAinda não há avaliações
- Crowns Used in Pediatric DentistrDocumento85 páginasCrowns Used in Pediatric DentistrShahid Shaikh100% (1)
- Non Surgical Endodontic Retreatment: Presented byDocumento58 páginasNon Surgical Endodontic Retreatment: Presented bySayak GuptaAinda não há avaliações
- Gnath OlogyDocumento41 páginasGnath Ologypushpavalli22100% (1)
- Biocreative OrthodonticsDocumento9 páginasBiocreative OrthodonticsManishPisarla100% (4)
- Biologically Oriented Preparation Technique For SurgicallyDocumento6 páginasBiologically Oriented Preparation Technique For SurgicallyAbdelrahman Galal100% (1)
- Biologically Oriented Preparation Technique For SurgicallyDocumento6 páginasBiologically Oriented Preparation Technique For SurgicallyAbdelrahman Galal100% (1)
- Introducing Dental ImplantsDocumento167 páginasIntroducing Dental ImplantsEdu EduAinda não há avaliações
- Lec 3&4Documento163 páginasLec 3&4Mohamed Ali AbdelhamedAinda não há avaliações
- Prosthetic Management of Implants Placed With The Socket-Shield TechniqueDocumento5 páginasProsthetic Management of Implants Placed With The Socket-Shield TechniqueRiya KvAinda não há avaliações
- Articulo 2 EndoDocumento11 páginasArticulo 2 EndoPedro Gonzalez DelgadoAinda não há avaliações
- Bhomavat 2009Documento8 páginasBhomavat 2009Jing XueAinda não há avaliações
- Dentistry - Broken File Tip 2Documento7 páginasDentistry - Broken File Tip 2rrkafg5242Ainda não há avaliações
- Fugazzotto ImmediateImplantPlacementMolarDocumento7 páginasFugazzotto ImmediateImplantPlacementMolarLozovan GregoryAinda não há avaliações
- Endodontic MishapsDocumento19 páginasEndodontic MishapsSayak GuptaAinda não há avaliações
- Prosthetic Management of Implants Placed With The Socket-Shield TechniqueDocumento6 páginasProsthetic Management of Implants Placed With The Socket-Shield TechniqueSofia LondoñoAinda não há avaliações
- The Socket-Shield Technique at Molar Sites: A Proof-Of-Principle Technique Report. C Schwimer Et Al. JPD 2018:5 (12) 56-60Documento33 páginasThe Socket-Shield Technique at Molar Sites: A Proof-Of-Principle Technique Report. C Schwimer Et Al. JPD 2018:5 (12) 56-60rajaniAinda não há avaliações
- Jurnal RADIO PDFDocumento4 páginasJurnal RADIO PDFCita ChotimahAinda não há avaliações
- Orthodontic Extrusion of Fractured Maxillary Lateral Incisor - A Case ReportDocumento4 páginasOrthodontic Extrusion of Fractured Maxillary Lateral Incisor - A Case ReportInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Esthetic Rehabilitation With A Cast Partial Denture: Case ReportDocumento4 páginasEsthetic Rehabilitation With A Cast Partial Denture: Case ReportMissyAinda não há avaliações
- M Ethodical Jacket Crown Preparation: JU LY 1953 Volume 47 - Number 1Documento5 páginasM Ethodical Jacket Crown Preparation: JU LY 1953 Volume 47 - Number 1Gebyar Denimadyasa RebekaAinda não há avaliações
- Ovate PDFDocumento11 páginasOvate PDFAriPratiwiAinda não há avaliações
- A Simplified Method For The Fabrication of Obturator:a Case ReportDocumento4 páginasA Simplified Method For The Fabrication of Obturator:a Case ReportinventionjournalsAinda não há avaliações
- 95 FullDocumento7 páginas95 FullRimAinda não há avaliações
- Tic Re Treatment Versus Tooth Extraction - David B RosenbergDocumento7 páginasTic Re Treatment Versus Tooth Extraction - David B RosenbergShereen RagabAinda não há avaliações
- Retrieval of Fractured Abutment Screw From The Implant 2Documento27 páginasRetrieval of Fractured Abutment Screw From The Implant 2nadeemAinda não há avaliações
- 11.endodontic MishapsDocumento27 páginas11.endodontic MishapsRiya JainAinda não há avaliações
- Endodontic Cavity PreparationDocumento166 páginasEndodontic Cavity Preparationagusaranp0% (1)
- Choosing A Pre-Adjusted Orthodontic Appliance Prescription For Anterior TeethDocumento7 páginasChoosing A Pre-Adjusted Orthodontic Appliance Prescription For Anterior TeethAadhirai GopinathAinda não há avaliações
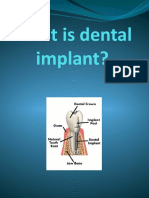
- What Is Dental ImplantDocumento14 páginasWhat Is Dental ImplantFaleh ZahrawiAinda não há avaliações
- Clinical: Use of Distal Implants To Support and Increase Retention of A Removable Partial Denture: A Case ReportDocumento4 páginasClinical: Use of Distal Implants To Support and Increase Retention of A Removable Partial Denture: A Case ReportDentist HereAinda não há avaliações
- Clinical Management of Aquired Defects of MaxillaDocumento81 páginasClinical Management of Aquired Defects of Maxillarayavarapu sunilAinda não há avaliações
- A Prosthodontic Rehabilitation of A Partial Maxillectomy Patient With Hollow Bulb ObturatorDocumento4 páginasA Prosthodontic Rehabilitation of A Partial Maxillectomy Patient With Hollow Bulb ObturatorDentist HereAinda não há avaliações
- Orthodontic Extrusion of Premolar Teeth - An Improved TechniqueDocumento6 páginasOrthodontic Extrusion of Premolar Teeth - An Improved TechniquejorgeAinda não há avaliações
- Case Report EndodonticsDocumento49 páginasCase Report EndodonticsFrancis PrathyushaAinda não há avaliações
- Implant QuizzesDocumento4 páginasImplant QuizzesBM 28 Stephanie Amelia Christanto, drgAinda não há avaliações
- 2007 - Intrusion of Overerupted Molars byDocumento7 páginas2007 - Intrusion of Overerupted Molars byTien Li AnAinda não há avaliações
- Imp 1Documento5 páginasImp 1pradeepgade1Ainda não há avaliações
- Case Report Band and Loop: A Case Report: Gurkiran Kaur, Garima ChoudharyDocumento6 páginasCase Report Band and Loop: A Case Report: Gurkiran Kaur, Garima Choudharyبسمة رياض عبد الستارAinda não há avaliações
- 2020 September by US Part2Documento129 páginas2020 September by US Part2Ahmed QahtaniAinda não há avaliações
- Apicoectomy of Palatal Root in Upper 1 Molar To Remove Endodontic Instrument: Rare Case ReportDocumento4 páginasApicoectomy of Palatal Root in Upper 1 Molar To Remove Endodontic Instrument: Rare Case ReportUmarsyah AliAinda não há avaliações
- A Rare Case of Periapical Healing in An Apically Extruding, Separated InstrumentDocumento3 páginasA Rare Case of Periapical Healing in An Apically Extruding, Separated InstrumentInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Re-Treatment: Case StudyDocumento3 páginasRe-Treatment: Case StudyodontogarayAinda não há avaliações
- Principles of Endodontic Surgery DR - YassirDocumento19 páginasPrinciples of Endodontic Surgery DR - YassirSRO oOAinda não há avaliações
- A To Z Orthodontics Vol 13 Fixed AppliancesDocumento31 páginasA To Z Orthodontics Vol 13 Fixed AppliancesMohammed NabeelAinda não há avaliações
- Awais AssignmentDocumento3 páginasAwais AssignmentMuhammad AwaisAinda não há avaliações
- Bioabsorbable Root Analogue For Closure of Oroantral Comm After Tooth ExtractionDocumento0 páginaBioabsorbable Root Analogue For Closure of Oroantral Comm After Tooth ExtractionTrinhTaAinda não há avaliações
- An 2/2 Implant Overdenture: Case ReportDocumento3 páginasAn 2/2 Implant Overdenture: Case ReportasclepiuspdfsAinda não há avaliações
- Clasificación Simpleficada de AlveólosDocumento7 páginasClasificación Simpleficada de AlveólosDaniel LazoAinda não há avaliações
- A P A O F S: Ndodontic Ccess Reparation N Pening OR UccessDocumento7 páginasA P A O F S: Ndodontic Ccess Reparation N Pening OR UccessHadil AltilbaniAinda não há avaliações
- ثDocumento40 páginasثZakria Al-HadadAinda não há avaliações
- Six Months of Tissue Healing and Conventional Dentures Procedures Is PreferableDocumento3 páginasSix Months of Tissue Healing and Conventional Dentures Procedures Is PreferableTiaraAinda não há avaliações
- Teeth in A Day Nys deDocumento4 páginasTeeth in A Day Nys deSatyendra KumarAinda não há avaliações
- With Row 1990Documento2 páginasWith Row 1990silpayAinda não há avaliações
- Intentional Replantation - A Last Resort Treatment or A Conventional Treatment Procedure Nine CasDocumento8 páginasIntentional Replantation - A Last Resort Treatment or A Conventional Treatment Procedure Nine CasFlorin IonescuAinda não há avaliações
- Periodontal Plastic Surgery For Esthetic Crown LengtheningDocumento4 páginasPeriodontal Plastic Surgery For Esthetic Crown LengtheningAbdelrahman GalalAinda não há avaliações
- Strengthening of A Model Composite RestorationDocumento9 páginasStrengthening of A Model Composite RestorationAbdelrahman GalalAinda não há avaliações
- Minimally Invasive Periodontal TherapyDocumento5 páginasMinimally Invasive Periodontal TherapyAbdelrahman GalalAinda não há avaliações
- Comparison of The Translucency of Two Mu PDFDocumento12 páginasComparison of The Translucency of Two Mu PDFAbdelrahman GalalAinda não há avaliações
- A Two-Stage Shape Optimization ProcessDocumento10 páginasA Two-Stage Shape Optimization ProcessAbdelrahman GalalAinda não há avaliações
- Transportation Assessment in Simulated CDocumento4 páginasTransportation Assessment in Simulated CAbdelrahman GalalAinda não há avaliações
- Adhesive Cementation of Indirect Composite Inlays and Onlays: A Literature ReviewDocumento9 páginasAdhesive Cementation of Indirect Composite Inlays and Onlays: A Literature ReviewAbdelrahman GalalAinda não há avaliações
- Fatigue Resistance and Failure Mode of eDocumento10 páginasFatigue Resistance and Failure Mode of eAbdelrahman GalalAinda não há avaliações
- All Ceramic Restorations (Why, When & HOW) : Dr. Mostafa NoorDocumento7 páginasAll Ceramic Restorations (Why, When & HOW) : Dr. Mostafa NoorAbdelrahman GalalAinda não há avaliações
- Intern Seminars FormDocumento13 páginasIntern Seminars FormAbdelrahman GalalAinda não há avaliações
- Questions For The State Exam in Therapeutic Dentistry Questions of Restorative DentistryDocumento8 páginasQuestions For The State Exam in Therapeutic Dentistry Questions of Restorative DentistryAbdelrahman GalalAinda não há avaliações
- Sealing Properties of One-Step Root-Filling Fibre Post-Obturators vs. Two-Step Delayed Fibre Post-PlacementDocumento6 páginasSealing Properties of One-Step Root-Filling Fibre Post-Obturators vs. Two-Step Delayed Fibre Post-PlacementAbdelrahman GalalAinda não há avaliações
- Sealing Properties of One-Step Root-Filling Fibre Post-Obturators vs. Two-Step Delayed Fibre Post-PlacementDocumento6 páginasSealing Properties of One-Step Root-Filling Fibre Post-Obturators vs. Two-Step Delayed Fibre Post-PlacementAbdelrahman GalalAinda não há avaliações
- Intracanal Cryotherapy Reduces PostoperaDocumento5 páginasIntracanal Cryotherapy Reduces PostoperaAbdelrahman GalalAinda não há avaliações
- Dentist Resume Example PDFDocumento1 páginaDentist Resume Example PDFAbdelrahman GalalAinda não há avaliações
- The Normal Periodontium Provides The Support Necessary To Maintain Teeth in FunctionDocumento19 páginasThe Normal Periodontium Provides The Support Necessary To Maintain Teeth in FunctionAbdelrahman GalalAinda não há avaliações
- Treatment of Mandibular Second Molar With S-Shaped Root CanalDocumento3 páginasTreatment of Mandibular Second Molar With S-Shaped Root CanalAbdelrahman GalalAinda não há avaliações
- Medical EmergenciesDocumento32 páginasMedical EmergenciesDharani Chowdary Kilari100% (1)
- FINAL Use and Application of Topical FluoridesDocumento7 páginasFINAL Use and Application of Topical FluoridesmahmoudAinda não há avaliações
- Non Carious Tooth Lesions Part 2Documento2 páginasNon Carious Tooth Lesions Part 2madssAinda não há avaliações
- Facebow Tech Spec Gen LRDocumento1 páginaFacebow Tech Spec Gen LRrojAinda não há avaliações
- Penatalaksanaan Gigi Premolar Kedua Maksila Dengan Saluran AKAR VERTUCCI TIPE V - Laporan KasusDocumento5 páginasPenatalaksanaan Gigi Premolar Kedua Maksila Dengan Saluran AKAR VERTUCCI TIPE V - Laporan KasuscrownAinda não há avaliações
- Chapter 8. Water FluoridationDocumento59 páginasChapter 8. Water FluoridationPutri Sundari100% (1)
- Oral Health Among Junior High School Student in Saints John and Paul Educational FoundationDocumento15 páginasOral Health Among Junior High School Student in Saints John and Paul Educational FoundationDat boiAinda não há avaliações
- 1-Pin Retained RestorationDocumento79 páginas1-Pin Retained Restorationemad helalAinda não há avaliações
- Poor Oral Health Including Active Caries in 187 UK Professional Male Football Players: Clinical Dental Examination Performed by DentistsDocumento6 páginasPoor Oral Health Including Active Caries in 187 UK Professional Male Football Players: Clinical Dental Examination Performed by DentistsJohnny CHAinda não há avaliações
- Pecial Tray and Final Impression: Special Tray (Individual or Custom TrayDocumento7 páginasPecial Tray and Final Impression: Special Tray (Individual or Custom TrayAatekaAinda não há avaliações
- Thesis On Oral HygieneDocumento87 páginasThesis On Oral Hygienesrijannagarkoti987Ainda não há avaliações
- SABC Medical Scheme Benefit Letter 2020Documento2 páginasSABC Medical Scheme Benefit Letter 2020Sibahle Zungu0% (1)
- Effect of Micro-Osteoperforations RatDocumento10 páginasEffect of Micro-Osteoperforations RatApurba SahariaAinda não há avaliações
- QS BJMP Lateral Entry 26 PositionsDocumento15 páginasQS BJMP Lateral Entry 26 PositionsreneresareyesAinda não há avaliações
- Multi-Distalizing Arch™ ApplianceDocumento4 páginasMulti-Distalizing Arch™ ApplianceOrtho OrganizersAinda não há avaliações
- Causes of Bad Breath (Halitosis)Documento13 páginasCauses of Bad Breath (Halitosis)Steven KauAinda não há avaliações
- The Domus Del Chirurgo at Rimini An Interim Account of The Medical AssemblageDocumento10 páginasThe Domus Del Chirurgo at Rimini An Interim Account of The Medical AssemblageMarie JuponAinda não há avaliações
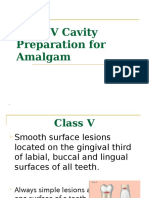
- Class VDocumento37 páginasClass VyahyaAinda não há avaliações
- Biomechanics of RPD 1Documento9 páginasBiomechanics of RPD 1Padmini ReddyAinda não há avaliações
- Antimicrobial Effectiveness of Cetylpyridinium Chloride and Zinc Chloride-Containing Mouthrinses On Bacteria of Halitosis and Peri-Implant DiseaseDocumento7 páginasAntimicrobial Effectiveness of Cetylpyridinium Chloride and Zinc Chloride-Containing Mouthrinses On Bacteria of Halitosis and Peri-Implant DiseasePhuong ThaoAinda não há avaliações
- Evidence Based Dentistry: Future Aspects: Short CommunicationDocumento5 páginasEvidence Based Dentistry: Future Aspects: Short CommunicationGarry B GunawanAinda não há avaliações
- Aspire Dental Academy Bonding ProtocolDocumento11 páginasAspire Dental Academy Bonding ProtocolCherifAinda não há avaliações
- An Orthopantomographic Study of Hypodontia in Permanent Teeth of Japanese Pediatric PatientsDocumento8 páginasAn Orthopantomographic Study of Hypodontia in Permanent Teeth of Japanese Pediatric PatientsMariaCristinaAinda não há avaliações