Você também pode gostar
- Epidemiological Study DesignsDocumento60 páginasEpidemiological Study DesignsAnn Hill100% (1)
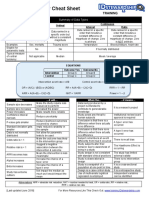
- Biostatistics Study Cheat SheetDocumento1 páginaBiostatistics Study Cheat Sheetab100% (1)
- PLE 2019 Preventive Medicine Answer KeyDocumento7 páginasPLE 2019 Preventive Medicine Answer Keydickson100% (1)
- Epidemiology in A Nutshell NCI BenchmarksDocumento8 páginasEpidemiology in A Nutshell NCI BenchmarksThe Nutrition CoalitionAinda não há avaliações
- Basic Concepts and Principles of EpidemiologyDocumento137 páginasBasic Concepts and Principles of EpidemiologyShubhamAinda não há avaliações
- Measures of AssociationDocumento56 páginasMeasures of AssociationAmsaluAinda não há avaliações
- Analytical epidemiology MCQs فراسDocumento12 páginasAnalytical epidemiology MCQs فراسHisokagen100% (1)
- Epidemiologic Methods: Confounding and Effect Modification: Distribution and MeasureDocumento30 páginasEpidemiologic Methods: Confounding and Effect Modification: Distribution and MeasureYong Hye JungAinda não há avaliações
- Lecture Notes On Epidemiology: The Aims of EpidemiologyDocumento11 páginasLecture Notes On Epidemiology: The Aims of Epidemiologysagar mittalAinda não há avaliações
- Interpretation and Choice of Effect Measures in Epidemiologic AnalysesDocumento8 páginasInterpretation and Choice of Effect Measures in Epidemiologic AnalysesAnnie WenAinda não há avaliações
- Prijono Satya Bakti Epidemiology Department University of AirlanggaDocumento29 páginasPrijono Satya Bakti Epidemiology Department University of AirlanggapuskesmasAinda não há avaliações
- Epidemiology Textbook NotesDocumento9 páginasEpidemiology Textbook NotesTaylor KohlmannAinda não há avaliações
- Critical Appraisal of Prognostic StudiesDocumento31 páginasCritical Appraisal of Prognostic StudiesInge Nolia Purwita SiwiAinda não há avaliações
- Desain Penelitian: SiswantoDocumento68 páginasDesain Penelitian: SiswantoPuti NoviandiniAinda não há avaliações
- Chapter 4 Case-Control StudyDocumento147 páginasChapter 4 Case-Control Studyaneleeemt7Ainda não há avaliações
- Epidemiological Studies: DR - Nisreen Mohammed Community MedicineDocumento24 páginasEpidemiological Studies: DR - Nisreen Mohammed Community MedicinehypopolaAinda não há avaliações
- Bioe 211 - Epidemiologic StudiesDocumento5 páginasBioe 211 - Epidemiologic Studiesbabalegaspi09Ainda não há avaliações
- Nciph ERIC5Documento6 páginasNciph ERIC5Obsinaan Olyke KefelegnAinda não há avaliações
- Probability: PSYB07 Gabriel Baylon October 2, 2013Documento9 páginasProbability: PSYB07 Gabriel Baylon October 2, 2013Gabriel BaylonAinda não há avaliações
- Analytical Epidemiology: Dr. Eman Khammas Al-Sadi Chief of Community DepartmentDocumento23 páginasAnalytical Epidemiology: Dr. Eman Khammas Al-Sadi Chief of Community DepartmentEman KhammasAinda não há avaliações
- Concept of Study Design in EpidemiologyDocumento48 páginasConcept of Study Design in Epidemiologyyulia.epidstudAinda não há avaliações
- Research Methodolgy 2: Dr. Ahmed GhandourDocumento29 páginasResearch Methodolgy 2: Dr. Ahmed Ghandourahmed tarekAinda não há avaliações
- Types of Research StudiesDocumento38 páginasTypes of Research Studiesنزار الحرازيAinda não há avaliações
- Recommended Reading Classification of Epidemiologic Study DesignsDocumento5 páginasRecommended Reading Classification of Epidemiologic Study DesignsTatiana SirbuAinda não há avaliações
- Coefficient of SkewnessDocumento89 páginasCoefficient of SkewnessAhsan KamranAinda não há avaliações
- EPIDemiologi BPK SiswantoDocumento47 páginasEPIDemiologi BPK SiswantoFachriza EffendiAinda não há avaliações
- Xie2011 IksDocumento11 páginasXie2011 IksDiego Alejandro Rojas MontanezAinda não há avaliações
- Research Design (Rancang Penelitian)Documento48 páginasResearch Design (Rancang Penelitian)Fachriza EffendiAinda não há avaliações
- Epidemiological Studies AND Methods in EpidemiologyDocumento83 páginasEpidemiological Studies AND Methods in Epidemiologysiva ranjini SureshAinda não há avaliações
- MPH EocDocumento8 páginasMPH EocGalaleldin AliAinda não há avaliações
- 12 Case Control Study DesignDocumento53 páginas12 Case Control Study DesignEldimson BermudoAinda não há avaliações
- The Problem of Multiple Testing - EncryptedDocumento6 páginasThe Problem of Multiple Testing - EncryptedDexter BraveAinda não há avaliações
- Study Desiegn 1Documento13 páginasStudy Desiegn 1Mian. Shoaib.Ainda não há avaliações
- Measures of Association: by Fisaha.H (Bsc. Mphil)Documento66 páginasMeasures of Association: by Fisaha.H (Bsc. Mphil)ruth100% (1)
- Measures of AssociationDocumento4 páginasMeasures of AssociationAastha jainAinda não há avaliações
- Virtual Reality Exposure Therapy For Panic DisordeDocumento1 páginaVirtual Reality Exposure Therapy For Panic Disordekhadija.temaraAinda não há avaliações
- BIOE Week 14Documento4 páginasBIOE Week 14FelicityAinda não há avaliações
- Lecture Notes (Level of Significance)Documento5 páginasLecture Notes (Level of Significance)Zearo GamingAinda não há avaliações
- Seminar 7Documento31 páginasSeminar 7David CoutinhoAinda não há avaliações
- Analysis of Cause Effect RelationshipDocumento50 páginasAnalysis of Cause Effect RelationshipRida AwwalAinda não há avaliações
- 6.3 Ecologic - Analysis PDFDocumento9 páginas6.3 Ecologic - Analysis PDFjmgt100Ainda não há avaliações
- Module 1Documento4 páginasModule 1Mc Philip Gabay DamoclesAinda não há avaliações
- Risk Assessment: Bruce CaseDocumento35 páginasRisk Assessment: Bruce CaseLion KhushiAinda não há avaliações
- Principles of Study Design in Environmental Epidemiology: Hal Morgenstern y Duncan ThomasDocumento17 páginasPrinciples of Study Design in Environmental Epidemiology: Hal Morgenstern y Duncan ThomasMaría José Balboa LopeteguiAinda não há avaliações
- Mathematical Modelling of Infectious DiseasesDocumento11 páginasMathematical Modelling of Infectious DiseasesBOBBY212Ainda não há avaliações
- Epidemiology: Basics of Study Design, Measures, and Limitations Defining EpidemiologyDocumento7 páginasEpidemiology: Basics of Study Design, Measures, and Limitations Defining EpidemiologyTariku AyeleAinda não há avaliações
- Epidemiology I (Recovered)Documento130 páginasEpidemiology I (Recovered)Lisa WiramasAinda não há avaliações
- Reproduction Numbers and Sub-Threshold Endemic Equilibria For Compartmental Models of Disease TransmissionDocumento20 páginasReproduction Numbers and Sub-Threshold Endemic Equilibria For Compartmental Models of Disease TransmissionSyahrani MuhammadAinda não há avaliações
- Notes On R: 1 The Basic Reproduction Number in A NutshellDocumento19 páginasNotes On R: 1 The Basic Reproduction Number in A Nutshelltotto pastimeAinda não há avaliações
- Media 64043 en PDFDocumento4 páginasMedia 64043 en PDFAbdelrahman M. AlnweiriAinda não há avaliações
- Dealing With The Coronavirus: Some Back of The Envelope CalculationsDocumento11 páginasDealing With The Coronavirus: Some Back of The Envelope CalculationsMauricio ZeaAinda não há avaliações
- 26 1605669892 3dhrnehmDocumento53 páginas26 1605669892 3dhrnehmSiska NovitaAinda não há avaliações
- Uncertainity in Probabilistic Risk AssessmentDocumento15 páginasUncertainity in Probabilistic Risk Assessmentchetan_7927Ainda não há avaliações
- 1127-1131 Rrijm180310228Documento5 páginas1127-1131 Rrijm180310228Sunil NegiAinda não há avaliações
- Risk Assessment IIDocumento4 páginasRisk Assessment IICristhian AdrianzenAinda não há avaliações
- Epidemiological Studies Eman Mahfouz 2022-1Documento81 páginasEpidemiological Studies Eman Mahfouz 2022-1ShriefElghazalyAinda não há avaliações
- Discrete and Continuous Dynamical Systems Series B Volume 14, Number 1, July 2010Documento23 páginasDiscrete and Continuous Dynamical Systems Series B Volume 14, Number 1, July 2010Daniel AscuntarAinda não há avaliações
- The Influenza A (H1N1) V Pandemic: An Exploratory System Dynamics ApproachDocumento33 páginasThe Influenza A (H1N1) V Pandemic: An Exploratory System Dynamics ApproachEgeruoh Chigoziri CyrinusAinda não há avaliações
- By-Dr. Oinam Monica DeviDocumento98 páginasBy-Dr. Oinam Monica DevimonikaAinda não há avaliações
- Study DesignsDocumento13 páginasStudy DesignsHassanAinda não há avaliações
- Epidemiology Final Exam Outline:: Exposures.?Documento33 páginasEpidemiology Final Exam Outline:: Exposures.?Farah FarahAinda não há avaliações
- Rule of Thumb in Sample SizesDocumento8 páginasRule of Thumb in Sample SizesBigs BigayAinda não há avaliações
- Lec-06 Analytical Study DesignsDocumento23 páginasLec-06 Analytical Study DesignsNinadNagraleAinda não há avaliações
- Measures of AssociationDocumento46 páginasMeasures of Associationkuchie ranksAinda não há avaliações
- Epidemiology: Presented By: DR Susan Abraham 1st Year PG Dept of PeriodonticsDocumento106 páginasEpidemiology: Presented By: DR Susan Abraham 1st Year PG Dept of PeriodonticsSusan AbrahamAinda não há avaliações
- Particle emission concept and probabilistic consideration of the development of infections in systems: Dynamics from logarithm and exponent in the infection process, percolation effectsNo EverandParticle emission concept and probabilistic consideration of the development of infections in systems: Dynamics from logarithm and exponent in the infection process, percolation effectsAinda não há avaliações
- Van Der Ven Susser 2023 Structural Racism and Risk of SchizophreniaDocumento3 páginasVan Der Ven Susser 2023 Structural Racism and Risk of SchizophreniaLink079Ainda não há avaliações
- Why The Neighborhood Social Environment Is Critical in Obesity PreventionDocumento7 páginasWhy The Neighborhood Social Environment Is Critical in Obesity PreventionLink079Ainda não há avaliações
- Addington Et Al-2018-Early Intervention in PsychiatryDocumento8 páginasAddington Et Al-2018-Early Intervention in PsychiatryLink079Ainda não há avaliações
- Changing Practice: Frameworks From Implementation ScienceDocumento4 páginasChanging Practice: Frameworks From Implementation ScienceLink079Ainda não há avaliações
- Solution To Tutorial 2: ST3241 Categorical Data Analysis I Semester II, 2010-2011Documento4 páginasSolution To Tutorial 2: ST3241 Categorical Data Analysis I Semester II, 2010-2011Griya AyuAinda não há avaliações
- Salm IDocumento24 páginasSalm IMiranti PuspasariAinda não há avaliações
- Lecture 4Documento45 páginasLecture 4PradeepAinda não há avaliações
- 10 Pharmacotherapy Vol 1 Study DesignsDocumento34 páginas10 Pharmacotherapy Vol 1 Study DesignsAnonymous oqvanOVAinda não há avaliações
- RMB DWDocumento20 páginasRMB DWDrAftab AhmedAinda não há avaliações
- Logistic Regression Mini TabDocumento20 páginasLogistic Regression Mini TabAnıl Toraman100% (2)
- EpicalcDocumento328 páginasEpicalcgaveninAinda não há avaliações
- The Four Most Common Types of Epidemiological StudiesDocumento10 páginasThe Four Most Common Types of Epidemiological Studiesdaniellab23Ainda não há avaliações
- Jurding DR Oyo PDFDocumento12 páginasJurding DR Oyo PDFAlfred hartoyoAinda não há avaliações
- Dietary and Environmental Determinants of Oesophageal CancerDocumento12 páginasDietary and Environmental Determinants of Oesophageal CancerBerhanuAinda não há avaliações
- Daftar PustakaDocumento43 páginasDaftar PustakaFeni Nurmia PutriAinda não há avaliações
- A Beginner's Guide To Interpreting Odds Ratios, Confidence Intervals and P-Values - Students 4 Best EvidenceDocumento35 páginasA Beginner's Guide To Interpreting Odds Ratios, Confidence Intervals and P-Values - Students 4 Best EvidenceABID ALIAinda não há avaliações
- Septiya Agestin Cahyaningrum - Resume of Disease Frequency MeasurementDocumento17 páginasSeptiya Agestin Cahyaningrum - Resume of Disease Frequency MeasurementSepty KawaiAinda não há avaliações
- Hsern Ern's UCS Exam Revision NotesDocumento10 páginasHsern Ern's UCS Exam Revision NotesNanthida AngAinda não há avaliações
- Disease Detectives NotesDocumento4 páginasDisease Detectives NotesOwen LiuAinda não há avaliações
- Germany CancerDocumento6 páginasGermany CancerDaniel VenablesAinda não há avaliações
- Bivariate Analysis of Sensitivity and Specificity Produces Informative Summary Measures in Diagnostic ReviewsDocumento12 páginasBivariate Analysis of Sensitivity and Specificity Produces Informative Summary Measures in Diagnostic ReviewsYeltsin CastroAinda não há avaliações
- RPH Letter Biostatistics ReviewDocumento14 páginasRPH Letter Biostatistics Reviewtpatel0986Ainda não há avaliações
- Washington's Drug Offender Sentencing Alternative: An Update On Recidivism FindingsDocumento8 páginasWashington's Drug Offender Sentencing Alternative: An Update On Recidivism FindingsWashington State Institute for Public Policy100% (1)
- PH150A Week 7 HWDocumento9 páginasPH150A Week 7 HWMegha BanerjeeAinda não há avaliações
- SPSS LiaDocumento8 páginasSPSS Liadilla ratnajAinda não há avaliações
- 4 - Analytical EpidemiologyDocumento20 páginas4 - Analytical EpidemiologyMuhammad Zubair Bhutta100% (1)
- Applied Statistics and The SAS ProgrammingDocumento85 páginasApplied Statistics and The SAS Programminganugupta.wj9719100% (1)
- A Review of The Application of Logistic RegressionDocumento58 páginasA Review of The Application of Logistic RegressionFrancisco ArteagaAinda não há avaliações