Você também pode gostar
- Appointment schedule template for a weekDocumento1 páginaAppointment schedule template for a weekMasrum SyamAinda não há avaliações
- Invoice: No: Physiotherapist: Date: Patient: Description Session Price Qty Amount DiagnoseDocumento2 páginasInvoice: No: Physiotherapist: Date: Patient: Description Session Price Qty Amount DiagnoseMasrum SyamAinda não há avaliações
- Keterangan JurnalDocumento1 páginaKeterangan JurnalMasrum SyamAinda não há avaliações
- Master Label UndanganDocumento1 páginaMaster Label UndanganMasrum SyamAinda não há avaliações
- Ankle ArthrosDocumento2 páginasAnkle ArthrosIoana HarpaAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- OpicDocumento17 páginasOpicKaren Roxas100% (1)
- British LeylandDocumento5 páginasBritish LeylandAnonymous DduElf20OAinda não há avaliações
- Juegos ps4Documento22 páginasJuegos ps4Gabriel CarvajalAinda não há avaliações
- Beyond 'Understanding' To Skilful Play in Games, Through Play PracticeDocumento12 páginasBeyond 'Understanding' To Skilful Play in Games, Through Play PracticeKelvin KohAinda não há avaliações
- Volvo CatalogDocumento44 páginasVolvo CataloghuurlingAinda não há avaliações
- KELTIS RulebookDocumento3 páginasKELTIS RulebookIsa R. AkbarAinda não há avaliações
- AFC Club Ranking 2011-2014: Top 100 Clubs by PointsDocumento2 páginasAFC Club Ranking 2011-2014: Top 100 Clubs by PointsSuraedi TambakAinda não há avaliações
- Punjab Public Service Commission, Lahore: NoticeDocumento5 páginasPunjab Public Service Commission, Lahore: NoticeWajid MahmoodAinda não há avaliações
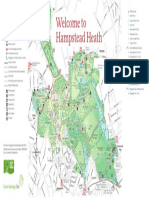
- Hampstead Heath MapDocumento1 páginaHampstead Heath MapKayla PadillaAinda não há avaliações
- Pico ChessDocumento18 páginasPico ChessEarthtopusAinda não há avaliações
- Inventory File 9.21.2022Documento120 páginasInventory File 9.21.2022EVGtruthAinda não há avaliações
- Bolt Action 3Documento10 páginasBolt Action 3browar444100% (2)
- GM TechLink 21 November 2022Documento9 páginasGM TechLink 21 November 2022River OzAinda não há avaliações
- 18 - MonarchDocumento1 página18 - MonarchBima MahendraAinda não há avaliações
- Marlene Sudtirol Sunshine Race 2024 - Iscritti HCDocumento9 páginasMarlene Sudtirol Sunshine Race 2024 - Iscritti HCMTB-VCOAinda não há avaliações
- 2013 LOOK Cycle Catalog USDocumento35 páginas2013 LOOK Cycle Catalog USeskewtAinda não há avaliações
- Target ShooterDocumento60 páginasTarget Shooterdevildgog100% (1)
- Stretching and Flexibility: How To StretchDocumento11 páginasStretching and Flexibility: How To StretchkontakcAinda não há avaliações
- BEML Motor GraderDocumento4 páginasBEML Motor GraderVivek AnandAinda não há avaliações
- Pure Love Chords: Guitar Tabs Updates News Reviews Interviews Columns Lessons Community Forums Contests UG. SlashDocumento4 páginasPure Love Chords: Guitar Tabs Updates News Reviews Interviews Columns Lessons Community Forums Contests UG. SlashmodigilianyAinda não há avaliações
- Stanza Stones Trail Guide Short Walk - MIST STONEDocumento2 páginasStanza Stones Trail Guide Short Walk - MIST STONEIlkley Literature FestivalAinda não há avaliações
- Nikon 2008 Hunting Optics CatalogDocumento52 páginasNikon 2008 Hunting Optics CatalogCraig ThompsonAinda não há avaliações
- Physical Rehabilitation 2.2 Rehabilitation of Lower Limb Musculoskeletal DisordersDocumento6 páginasPhysical Rehabilitation 2.2 Rehabilitation of Lower Limb Musculoskeletal DisordersJAIRISH YZABELLE SALVADORAinda não há avaliações
- Defaulter List-Software EngineeringDocumento14 páginasDefaulter List-Software Engineeringchatgpt0316540Ainda não há avaliações
- Muscle & Fitness Hers - August 2016Documento132 páginasMuscle & Fitness Hers - August 2016Fitness Fits Me100% (3)
- Parts Manual: GS-2032 GS-2632 GS-3232Documento219 páginasParts Manual: GS-2032 GS-2632 GS-3232J. Eduardo Montoya S.Ainda não há avaliações
- Swarms TemplateDocumento2 páginasSwarms TemplateGabrielle Matt CostelloAinda não há avaliações
- Fundamental RhythmDocumento27 páginasFundamental RhythmJohn Luis MolanoAinda não há avaliações
- OBC-TGB-UN01-ER007 (2 OF 2) - Rev 3aDocumento1 páginaOBC-TGB-UN01-ER007 (2 OF 2) - Rev 3akninstruments2Ainda não há avaliações
- Dunlop Tires Catalog PDFDocumento85 páginasDunlop Tires Catalog PDFRobertAinda não há avaliações