Você também pode gostar
- Self Assessment in Musculoskeletal Pathology X-raysNo EverandSelf Assessment in Musculoskeletal Pathology X-raysNota: 5 de 5 estrelas5/5 (2)
- 1320 Arthritis Mutilans As A Radiographic Feature of Systemic Sclerosis FileDocumento2 páginas1320 Arthritis Mutilans As A Radiographic Feature of Systemic Sclerosis FileNikita KhmelinskiiAinda não há avaliações
- Conventional Radiology in Rheumatoid ArthritisDocumento26 páginasConventional Radiology in Rheumatoid ArthritisDanAinda não há avaliações
- Cervical Rheumatoid Nodule Mimicking A Lymph Node: Abdulrahman A. Khormi, Lama A. Al-Hmaly, Abdulrahman AlarfajDocumento4 páginasCervical Rheumatoid Nodule Mimicking A Lymph Node: Abdulrahman A. Khormi, Lama A. Al-Hmaly, Abdulrahman AlarfajijasrjournalAinda não há avaliações
- Collagenous Fibroma (Desmoplastic Fibroblastoma) : Clinical, Pathological and Imaging FindingsDocumento41 páginasCollagenous Fibroma (Desmoplastic Fibroblastoma) : Clinical, Pathological and Imaging FindingsAnonymous bE4VegCcAinda não há avaliações
- Giant Cell Tumor of The Tendon Sheath: A Rare Case in The Left Knee of A 15-Year-Old BoyDocumento3 páginasGiant Cell Tumor of The Tendon Sheath: A Rare Case in The Left Knee of A 15-Year-Old BoyFriadi NataAinda não há avaliações
- Diagnostic Difficulties in Fibrous Dysplasia - A 5-Case Series and A Literature ReviewDocumento9 páginasDiagnostic Difficulties in Fibrous Dysplasia - A 5-Case Series and A Literature Reviewsolikin ikinAinda não há avaliações
- Nelson EWDocumento6 páginasNelson EWDewidewidewi Madridista Part IIAinda não há avaliações
- Hon 2005Documento2 páginasHon 2005Andana TrisaviAinda não há avaliações
- Sajr 22 1316Documento6 páginasSajr 22 1316Nafiatul MuasyarahAinda não há avaliações
- Extra Renal Rhabdoid Tumor in An Adult Presentin 2024 International JournalDocumento5 páginasExtra Renal Rhabdoid Tumor in An Adult Presentin 2024 International JournalRonald QuezadaAinda não há avaliações
- Aneurysmal Bone CystDocumento5 páginasAneurysmal Bone CystDipti PatilAinda não há avaliações
- Progressive Onset of Low Back Pain: Unusual Imaging Findings On CT and MriDocumento3 páginasProgressive Onset of Low Back Pain: Unusual Imaging Findings On CT and MriAloysius Wahyu LaspaRoAinda não há avaliações
- Tolosa-Hunt Syndrome in Double-Hit Lymphoma: Case Reports in Oncological Medicine March 2015Documento6 páginasTolosa-Hunt Syndrome in Double-Hit Lymphoma: Case Reports in Oncological Medicine March 2015Elisabeth TikalakaAinda não há avaliações
- Giant Solitary Cutaneous Angiosarcoma of The Forearm Occurring Outside The Setting of LymphedemaDocumento5 páginasGiant Solitary Cutaneous Angiosarcoma of The Forearm Occurring Outside The Setting of LymphedemaIJAR JOURNALAinda não há avaliações
- 10.1007@s00277 020 04011 8Documento2 páginas10.1007@s00277 020 04011 8cronoss21Ainda não há avaliações
- 2002 17 3 181 185 EngDocumento5 páginas2002 17 3 181 185 EngMortezaAinda não há avaliações
- Intrathyroidal Lymphoepithelial (Branchial) Cyst: Diagnostic and Management Challenge of A Rare EntityDocumento5 páginasIntrathyroidal Lymphoepithelial (Branchial) Cyst: Diagnostic and Management Challenge of A Rare EntityMeliAinda não há avaliações
- A Rare Case of Space Occupying Lesion of Brainstem in An Elderly Male PatientDocumento3 páginasA Rare Case of Space Occupying Lesion of Brainstem in An Elderly Male PatientInternational Journal of Clinical and Biomedical Research (IJCBR)Ainda não há avaliações
- Someunusualparaneoplasticsyndromes: Diagnosis in OncologyDocumento6 páginasSomeunusualparaneoplasticsyndromes: Diagnosis in OncologyMohamed Nuri ShembeshAinda não há avaliações
- Intraosseous Arteriovenous Malformations Mimicking Malignant DiseaseDocumento7 páginasIntraosseous Arteriovenous Malformations Mimicking Malignant DiseaseNm SAinda não há avaliações
- A Rare Case of Large Size Undifferentiated Pleomorphic Sarcoma of AnkleDocumento5 páginasA Rare Case of Large Size Undifferentiated Pleomorphic Sarcoma of AnkleIJAR JOURNALAinda não há avaliações
- J500210089 Muhammad Rizqy Noer Tuanaya Tugas Jurnal Bahasa Indonesia 2022Documento14 páginasJ500210089 Muhammad Rizqy Noer Tuanaya Tugas Jurnal Bahasa Indonesia 2022kiki tuanaya1Ainda não há avaliações
- Raval PDFDocumento5 páginasRaval PDFdebby claudiAinda não há avaliações
- Dermatomyositis and Undifferentiated Nasopharyngeal Carcinoma. A Rare Presentation of A Rare MalignancyDocumento4 páginasDermatomyositis and Undifferentiated Nasopharyngeal Carcinoma. A Rare Presentation of A Rare MalignancyasclepiuspdfsAinda não há avaliações
- 1 s2.0 S2049080122008718 MainDocumento4 páginas1 s2.0 S2049080122008718 MainFarizka Dwinda HidayatAinda não há avaliações
- Yamada 2010Documento5 páginasYamada 2010valeria lindaAinda não há avaliações
- Case Report: Zehava Sadka Rosenberg, 1 Steven Shankman, 1 Michael Klein, 2'3 and Wallace Lehman4Documento3 páginasCase Report: Zehava Sadka Rosenberg, 1 Steven Shankman, 1 Michael Klein, 2'3 and Wallace Lehman4Mohamed Ali Al-BuflasaAinda não há avaliações
- Cemento-Osseous DysplasiaDocumento5 páginasCemento-Osseous DysplasiaFatima AliAinda não há avaliações
- Lapsus Ortho Word - Id.enDocumento17 páginasLapsus Ortho Word - Id.eninhaAinda não há avaliações
- Anaplastic Large Cell Lymphoma Alk Negative of The Mandible As The First Clinical Manifestation of Acquired Immunodeficiency SyndromeDocumento5 páginasAnaplastic Large Cell Lymphoma Alk Negative of The Mandible As The First Clinical Manifestation of Acquired Immunodeficiency SyndromeIJAR JOURNALAinda não há avaliações
- Traumatic Bone Cyst of Idiopathic Origin? A Report of Two CasesDocumento5 páginasTraumatic Bone Cyst of Idiopathic Origin? A Report of Two CasesjulietAinda não há avaliações
- Case Report: Langerhans Cell Histiocytosis of The Mandible in A Six-Year-Old ChildDocumento0 páginaCase Report: Langerhans Cell Histiocytosis of The Mandible in A Six-Year-Old ChildElvina Agnestin HarianjaAinda não há avaliações
- Tuberculosis of The Patella, Report CaseDocumento4 páginasTuberculosis of The Patella, Report CaseAnonymous AzXah9n0YAinda não há avaliações
- Spastic Quadraparesis Following A Relatively Minor Injury - The Os Odontoideum'Documento3 páginasSpastic Quadraparesis Following A Relatively Minor Injury - The Os Odontoideum'Stefan StanciuAinda não há avaliações
- Calcific Tendinitis of The Rotator Cuff State of The Art in Diagnosis PDFDocumento8 páginasCalcific Tendinitis of The Rotator Cuff State of The Art in Diagnosis PDFItai IzhakAinda não há avaliações
- Unusual Clinicoradiographic Presentation of A Lateral Periodontal CystDocumento5 páginasUnusual Clinicoradiographic Presentation of A Lateral Periodontal CystTzitzi FloresAinda não há avaliações
- Journal of Oral and Maxillofacial Surgery, Medicine, and PathologyDocumento7 páginasJournal of Oral and Maxillofacial Surgery, Medicine, and PathologyOMFS FKG UnimusAinda não há avaliações
- Linfoma Extranodal en Cabeaza y CuelloDocumento5 páginasLinfoma Extranodal en Cabeaza y CuelloCARLOS DARIO MERINO BUSTAMANTEAinda não há avaliações
- Long Survival With Metastatic Clear Cell Sarcoma of The Achilles Tendon JFAS 1996Documento5 páginasLong Survival With Metastatic Clear Cell Sarcoma of The Achilles Tendon JFAS 1996Evan BowlesAinda não há avaliações
- 03-Arthritis and Connective Tissue DisordersDocumento19 páginas03-Arthritis and Connective Tissue DisordersKhiara Yapha AlfarAinda não há avaliações
- DescargaDocumento8 páginasDescargaFrancis ValdiviaAinda não há avaliações
- Isolated Lesser Trochanter Fracture Associated With LeukemiaDocumento3 páginasIsolated Lesser Trochanter Fracture Associated With LeukemiaIndora DenniAinda não há avaliações
- Merolla 2015Documento8 páginasMerolla 2015Sandro RolimAinda não há avaliações
- CR - RamirezDocumento4 páginasCR - RamirezTommysAinda não há avaliações
- Idiopathic Stroke After Syndromic and Neuromuscular Scoliosis Surgery: A Case Report and Literature ReviewDocumento7 páginasIdiopathic Stroke After Syndromic and Neuromuscular Scoliosis Surgery: A Case Report and Literature ReviewflashjetAinda não há avaliações
- Lhermitte Duclos Disease - A Case Report: Ramya C, Renuka IV, Durga Prasad B, Pratyusha NDocumento4 páginasLhermitte Duclos Disease - A Case Report: Ramya C, Renuka IV, Durga Prasad B, Pratyusha NajmrdAinda não há avaliações
- Skeletal GB Mimant SarcomeDocumento7 páginasSkeletal GB Mimant Sarcomeal qurtubi al andalusiAinda não há avaliações
- A Rare Case of Retroperitoneal and Mesenteric LymphangiomatosisDocumento4 páginasA Rare Case of Retroperitoneal and Mesenteric LymphangiomatosisAndra KurniantoAinda não há avaliações
- Romano Et Al 2020 Solitary Fibrous Tumor of The Deep Parotid GlandDocumento3 páginasRomano Et Al 2020 Solitary Fibrous Tumor of The Deep Parotid GlandReyes Ivan García CuevasAinda não há avaliações
- EN + EosinofiliaDocumento3 páginasEN + EosinofiliaAna Flavia BaptistaAinda não há avaliações
- Nassera Pnet PDFDocumento5 páginasNassera Pnet PDFMuneer KhalamAinda não há avaliações
- A Giant Plexiform Schwannoma of The Brachial Plexus: Case ReportDocumento6 páginasA Giant Plexiform Schwannoma of The Brachial Plexus: Case ReportpetrarizkyAinda não há avaliações
- Artritis Reumatoride y AnestesiaDocumento7 páginasArtritis Reumatoride y Anestesiamacielhinostroza9006Ainda não há avaliações
- Rheumatoid Arthritis and AnaesthesiaDocumento7 páginasRheumatoid Arthritis and AnaesthesiaAbante_gammaAinda não há avaliações
- Parosteal Lipoma of Proximal Radius A Rare Case ReDocumento4 páginasParosteal Lipoma of Proximal Radius A Rare Case ReKRISHNA19651Ainda não há avaliações
- Case Report BM 1Documento6 páginasCase Report BM 1Mohamad BasofiAinda não há avaliações
- Case On Ankle SurgeryDocumento13 páginasCase On Ankle SurgeryLuqman AhmedAinda não há avaliações
- Primary Osteosarcoma of The Nasal Fossa: An Exceptional PresentationDocumento5 páginasPrimary Osteosarcoma of The Nasal Fossa: An Exceptional PresentationRian HasniAinda não há avaliações
- Introduction To Smoking MeatDocumento2 páginasIntroduction To Smoking MeatrexaAinda não há avaliações
- Trees and Their ImportanceDocumento13 páginasTrees and Their ImportancerexaAinda não há avaliações
- Introduction To Corned BeefDocumento4 páginasIntroduction To Corned BeefrexaAinda não há avaliações
- Tuna and Its Steps of ProcessingDocumento17 páginasTuna and Its Steps of ProcessingrexaAinda não há avaliações
- Sustainability For The GamesDocumento42 páginasSustainability For The GamesrexaAinda não há avaliações
- How To Build An Effective FMCG Distribution System Through Collaboration Between Industry and TradeDocumento42 páginasHow To Build An Effective FMCG Distribution System Through Collaboration Between Industry and TraderexaAinda não há avaliações
- Stars and Their Basic PropertiesDocumento29 páginasStars and Their Basic PropertiesrexaAinda não há avaliações
- A Paper On Mad Cow Disease and Variant Creutzfeldt Jakob DiseaseDocumento22 páginasA Paper On Mad Cow Disease and Variant Creutzfeldt Jakob DiseaserexaAinda não há avaliações
- Info On DinosaursDocumento40 páginasInfo On DinosaursrexaAinda não há avaliações
- A History of Scientology Explained by Pictures (Drawings)Documento42 páginasA History of Scientology Explained by Pictures (Drawings)rexaAinda não há avaliações
- Ebola Virus.... Its Characteristics and ImpactDocumento29 páginasEbola Virus.... Its Characteristics and ImpactrexaAinda não há avaliações
- About Washing MachineDocumento22 páginasAbout Washing MachinerexaAinda não há avaliações
- Chapter 1 Pharmacognosy IntroductionDocumento47 páginasChapter 1 Pharmacognosy IntroductionrexaAinda não há avaliações
- A Presentation On The Medication.. CARBAMAZEPINEDocumento30 páginasA Presentation On The Medication.. CARBAMAZEPINErexaAinda não há avaliações
- All About Calendar (For Preschoolers)Documento41 páginasAll About Calendar (For Preschoolers)rexaAinda não há avaliações
- Prions Its Structure and HistoryDocumento28 páginasPrions Its Structure and HistoryrexaAinda não há avaliações
- A Seminar About The Rundown On MERS-COVDocumento45 páginasA Seminar About The Rundown On MERS-COVrexaAinda não há avaliações
- Electric Fan Consumer ElectronicsDocumento53 páginasElectric Fan Consumer ElectronicsrexaAinda não há avaliações
- The History of Clocks (For Elementary)Documento10 páginasThe History of Clocks (For Elementary)rexaAinda não há avaliações
- Introduction To Infectious Diseases and Bacterial InfectionsDocumento91 páginasIntroduction To Infectious Diseases and Bacterial InfectionsrexaAinda não há avaliações
- Poetry Writing Getting StartedDocumento12 páginasPoetry Writing Getting StartedrexaAinda não há avaliações
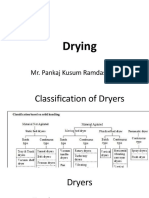
- Dryers Used in ProductionDocumento28 páginasDryers Used in ProductionrexaAinda não há avaliações
- Surgical Pathology of Liver and GallbladderDocumento55 páginasSurgical Pathology of Liver and GallbladderrexaAinda não há avaliações
- Surgical Pathology of Hepatobiliary Tree and PancreasDocumento53 páginasSurgical Pathology of Hepatobiliary Tree and PancreasrexaAinda não há avaliações
- Recurrent Vomiting PediatricsDocumento42 páginasRecurrent Vomiting PediatricsrexaAinda não há avaliações
- Liver Abscess - Its Pathophysiology and ManagementDocumento34 páginasLiver Abscess - Its Pathophysiology and ManagementrexaAinda não há avaliações
- Laparoendoscopic Single Site Surgery For Management of Heterotopic Pregnancy A Case Report and Review of LiteratureDocumento7 páginasLaparoendoscopic Single Site Surgery For Management of Heterotopic Pregnancy A Case Report and Review of LiteraturerexaAinda não há avaliações
- Trauma of Area of Chest Operation Powerpoint PresentationDocumento128 páginasTrauma of Area of Chest Operation Powerpoint PresentationrexaAinda não há avaliações
- Drugs & Pharmaceuticals PRESENTATIONDocumento30 páginasDrugs & Pharmaceuticals PRESENTATIONrexaAinda não há avaliações
- Professionals and Practitioners in CounselingDocumento20 páginasProfessionals and Practitioners in CounselingJac KieAinda não há avaliações
- Healing ArchitectureDocumento5 páginasHealing ArchitectureSUDHAKARMANI100% (2)
- Albuterol Pediatric Drug CardDocumento2 páginasAlbuterol Pediatric Drug CardAnthonyMedinaAinda não há avaliações
- How To Use Eye Drops ProperlyDocumento9 páginasHow To Use Eye Drops ProperlyQoshrina AdenitaAinda não há avaliações
- Memorandum of Decision of The Honourable Madam Justice S.L. MartinDocumento20 páginasMemorandum of Decision of The Honourable Madam Justice S.L. MartincalcitydeskAinda não há avaliações
- Friday Problem Statement PresentationDocumento7 páginasFriday Problem Statement PresentationyashramawatAinda não há avaliações
- Brittany 2Documento4 páginasBrittany 2Sharon Williams75% (4)
- Expert Consensus On The Desirable Characteristics of Review Criteria For Improvement of Health Care QualityDocumento6 páginasExpert Consensus On The Desirable Characteristics of Review Criteria For Improvement of Health Care Qualityujangketul62Ainda não há avaliações
- Chronic Kidney Disease Clinical Presentation - History, Physical ExaminationDocumento2 páginasChronic Kidney Disease Clinical Presentation - History, Physical ExaminationBayu Surya DanaAinda não há avaliações
- MAHONY, Patrick - The Boundaries of Free AssociationDocumento34 páginasMAHONY, Patrick - The Boundaries of Free AssociationPelículasVeladasAinda não há avaliações
- Pharmacology of Local Anesthetics IDocumento93 páginasPharmacology of Local Anesthetics IAlshaimaa AhmedAinda não há avaliações
- Medical CenterDocumento38 páginasMedical CenterKhea Micole MayAinda não há avaliações
- Charting by ExceptionDocumento7 páginasCharting by Exceptionafini aninditaAinda não há avaliações
- 021218drug Study CetirizineDocumento2 páginas021218drug Study Cetirizineliza sian100% (1)
- Dr. Robert Tirtowijoyo (Paediatric Condition) Inggris UMJ Maret 2008Documento73 páginasDr. Robert Tirtowijoyo (Paediatric Condition) Inggris UMJ Maret 2008Muhamad Agung SupriyantoAinda não há avaliações
- Director Quality Risk Management in Western MA Resume Stanley KoniecznyDocumento2 páginasDirector Quality Risk Management in Western MA Resume Stanley KoniecznyStanley KoniecznyAinda não há avaliações
- First Aid Pharmacology AntimicrobialsDocumento23 páginasFirst Aid Pharmacology AntimicrobialsLaura Lopez RocaAinda não há avaliações
- Imci Case StudyDocumento10 páginasImci Case StudyRhika Mae Flores Valdez100% (1)
- Paidepally Srinivas RaoDocumento9 páginasPaidepally Srinivas RaoShyam KalavalapalliAinda não há avaliações
- Epilepsy SurgeryDocumento13 páginasEpilepsy SurgeryDon RomanAinda não há avaliações
- IPOL Package InsertDocumento28 páginasIPOL Package InsertHeather X RhodesAinda não há avaliações
- TFN Joyce TravelbeeDocumento33 páginasTFN Joyce Travelbeechryss advinculaAinda não há avaliações
- Dematologist Appointment Abhishekdixit 22oct5.20pmdigital RegistrarDocumento1 páginaDematologist Appointment Abhishekdixit 22oct5.20pmdigital RegistrarabhishekAinda não há avaliações
- Nursing Diagnosis of Prostate CancerDocumento3 páginasNursing Diagnosis of Prostate CancerSyafiqAzizi100% (1)
- Hearing LossDocumento9 páginasHearing Lossvicky singhAinda não há avaliações
- PneumothoraxDocumento14 páginasPneumothoraxAsterlita WenasAinda não há avaliações
- AnisokoriaDocumento5 páginasAnisokoriaNurunnisa IsnyAinda não há avaliações
- Chiari Malformation / Syringomyelia SchemeDocumento4 páginasChiari Malformation / Syringomyelia SchemeMihai SavescuAinda não há avaliações
- Children-Mental Health-Facts-NamiDocumento1 páginaChildren-Mental Health-Facts-Namiapi-298799918Ainda não há avaliações
- Pearls in PPCDocumento5 páginasPearls in PPCRajinder Kumar BassanAinda não há avaliações