Você também pode gostar
- The Diagnostic Accuracy of Abdominal Ultrasound Imaging For Detection of Ovarian MassesDocumento5 páginasThe Diagnostic Accuracy of Abdominal Ultrasound Imaging For Detection of Ovarian MassesHanny TanzilAinda não há avaliações
- The Diagnostic Accuracy of PDFDocumento5 páginasThe Diagnostic Accuracy of PDFfrnsskAinda não há avaliações
- Comparison of Ultrasound and Mammography For Early DiagnosisDocumento8 páginasComparison of Ultrasound and Mammography For Early Diagnosishdh1224Ainda não há avaliações
- Ijcmr 1184 Dec 28Documento3 páginasIjcmr 1184 Dec 28BayuHernawanRahmatMuhariaAinda não há avaliações
- Tiwari 2017Documento3 páginasTiwari 2017Dewa OkaAinda não há avaliações
- MedicineDocumento6 páginasMedicineJEAN CARLOS GALLO VALVERDEAinda não há avaliações
- Эластография 1Documento8 páginasЭластография 1Роман КлоковAinda não há avaliações
- Eficacia Diagnóstica de La Ecografía de Alta Resolución en La Diferenciación Entre Nódulos de Mama Benignos y MalignosDocumento13 páginasEficacia Diagnóstica de La Ecografía de Alta Resolución en La Diferenciación Entre Nódulos de Mama Benignos y MalignosKatherinne Sutizal100% (1)
- Cancer de MamaDocumento11 páginasCancer de MamaIng SánchezAinda não há avaliações
- Elasto Mama - JUm 2009Documento8 páginasElasto Mama - JUm 2009cjijcAinda não há avaliações
- Fa Lomo 2018Documento6 páginasFa Lomo 2018Mateus CespedesAinda não há avaliações
- Diagnostic Parameters To Differentiate Benign From Malignant Ovarian Masses With Contrast-Enhanced Transvaginal SonographyDocumento8 páginasDiagnostic Parameters To Differentiate Benign From Malignant Ovarian Masses With Contrast-Enhanced Transvaginal SonographyRush32Ainda não há avaliações
- Easjrit 54 95-102Documento10 páginasEasjrit 54 95-102readresearchpublicationsAinda não há avaliações
- Imaging of The Female Pelvis: ReviewDocumento11 páginasImaging of The Female Pelvis: ReviewDian Putri NingsihAinda não há avaliações
- Clinical Practice GuidelinesDocumento17 páginasClinical Practice GuidelinesPLM 51st National ConventionAinda não há avaliações
- Breast Cancer Missed at Screening Hindsight or MiDocumento6 páginasBreast Cancer Missed at Screening Hindsight or MideaAinda não há avaliações
- Iota PicoDocumento27 páginasIota Picoarcita hanjaniAinda não há avaliações
- Peprah 2018Documento7 páginasPeprah 2018Dewa OkaAinda não há avaliações
- Impact of Knowledge and AttituDocumento23 páginasImpact of Knowledge and AttituAnis SolikahAinda não há avaliações
- Omidiji 2017Documento7 páginasOmidiji 2017Dewa OkaAinda não há avaliações
- Posters: Postersession1:Obstetrics-Firsttrimester, GynecologyDocumento30 páginasPosters: Postersession1:Obstetrics-Firsttrimester, GynecologyJuniece Marie CastañedaAinda não há avaliações
- In General, Ultrasonography and Mammography Have Almost The Same Accuracy To Diagnose Mammary Neoplasms (Benign / Malignant)Documento7 páginasIn General, Ultrasonography and Mammography Have Almost The Same Accuracy To Diagnose Mammary Neoplasms (Benign / Malignant)Kereta KecilAinda não há avaliações
- Kiran sapru-NEWDocumento4 páginasKiran sapru-NEWEvelyn ChacónAinda não há avaliações
- Possibilities of Modern Radiation Methods of Breast PathologyDocumento12 páginasPossibilities of Modern Radiation Methods of Breast PathologyCentral Asian StudiesAinda não há avaliações
- Diagnostic Performance of International Ovarian Tumor Analysis IotaDocumento7 páginasDiagnostic Performance of International Ovarian Tumor Analysis IotaVon HippoAinda não há avaliações
- 10 18621-Eurj 1022192-2075884Documento6 páginas10 18621-Eurj 1022192-2075884mhariskurniawanAinda não há avaliações
- Trends in Delayed Breast Cancer Diagnosis After ReDocumento9 páginasTrends in Delayed Breast Cancer Diagnosis After ReeugeniaAinda não há avaliações
- Jum2015342207 PDF Jsessionid f04t01Documento11 páginasJum2015342207 PDF Jsessionid f04t01Al RawdhaAinda não há avaliações
- Ahmadinejad 20Documento8 páginasAhmadinejad 20ayuAinda não há avaliações
- Artikel Penelitian AldyDocumento13 páginasArtikel Penelitian AldyJufri aldyAinda não há avaliações
- Gulbahce 2016Documento5 páginasGulbahce 2016Valir HusleAinda não há avaliações
- Comparative Study of Fine Needle Aspiration Cytology and Histopathology in Grading Breast CarcinomaDocumento5 páginasComparative Study of Fine Needle Aspiration Cytology and Histopathology in Grading Breast CarcinomaMafazi RifqiAinda não há avaliações
- Four Risk of Malignancy Indices in Evaluation of Pelvic MassesDocumento8 páginasFour Risk of Malignancy Indices in Evaluation of Pelvic MassesherryAinda não há avaliações
- Predicting The Risk of Malignancy in Adnexal Masses Based On IOTA AJOG 2016Documento14 páginasPredicting The Risk of Malignancy in Adnexal Masses Based On IOTA AJOG 2016Fernando Suarez ChumaceroAinda não há avaliações
- Endoscopic Ultrasound and Early Diagnosis of Pancreatic CancerDocumento4 páginasEndoscopic Ultrasound and Early Diagnosis of Pancreatic CancerAchmad Dzulfikar AziziAinda não há avaliações
- AdenomiosDocumento7 páginasAdenomiosMauricio Ordaz RtkAinda não há avaliações
- 1 s2.0 S1110036217300481 MainDocumento3 páginas1 s2.0 S1110036217300481 MainPutri YingAinda não há avaliações
- Radiology RadiologyDocumento6 páginasRadiology RadiologyJonathan ReinaldoAinda não há avaliações
- 10 1016@j Bpobgyn 2015 11 014Documento17 páginas10 1016@j Bpobgyn 2015 11 014Marco Julcamoro AsencioAinda não há avaliações
- Ultrasound in Gynecology and ObstetricsDocumento197 páginasUltrasound in Gynecology and ObstetricsAli Murtaza AbbasAinda não há avaliações
- JR Fer IiiDocumento37 páginasJR Fer IiimhariskurniawanAinda não há avaliações
- DiagnoDocumento6 páginasDiagnoYuliaAinda não há avaliações
- Fonc 10 01353Documento11 páginasFonc 10 01353Nike KomalaAinda não há avaliações
- Duque Ortiz2020Documento8 páginasDuque Ortiz2020elorenAinda não há avaliações
- Der Chi 2001Documento19 páginasDer Chi 20013bood.3raqAinda não há avaliações
- (2017) - Management and Prognosis of Ovarian Yolk Sac Tumors An Analysis of The National Cancer Data BaseDocumento6 páginas(2017) - Management and Prognosis of Ovarian Yolk Sac Tumors An Analysis of The National Cancer Data Basehop truongvanAinda não há avaliações
- Proof: Gynecologic OncologyDocumento2 páginasProof: Gynecologic OncologyCamilaBurgosAinda não há avaliações
- Cervical CancerDocumento14 páginasCervical CancerAlejandra MurilloAinda não há avaliações
- Ovarian Masses: Surgery or Surveillance?Documento9 páginasOvarian Masses: Surgery or Surveillance?MutianbllAinda não há avaliações
- Evaluation of Breast Masses Using Mammography and Sonography As First Line InvestigationsDocumento3 páginasEvaluation of Breast Masses Using Mammography and Sonography As First Line InvestigationsNata SanjayaAinda não há avaliações
- Metastatic Behavior of Breast Cancer Subtypes: Ournal of Linical NcologyDocumento7 páginasMetastatic Behavior of Breast Cancer Subtypes: Ournal of Linical NcologyJafet Gonzalez EstradaAinda não há avaliações
- Liver MassesDocumento13 páginasLiver MasseslydiaAinda não há avaliações
- EJMCM Volume 9 Issue 3 Pages 5223-5231Documento9 páginasEJMCM Volume 9 Issue 3 Pages 5223-5231Saudamini NaikAinda não há avaliações
- Confounding Factors of Transvaginal UltrasoundDocumento7 páginasConfounding Factors of Transvaginal UltrasoundYoshi RiantyokoAinda não há avaliações
- Exact ArticleDocumento6 páginasExact ArticleMuhammad WaqasAinda não há avaliações
- The Benefit of Tru-Cut Biopsy in Breast Masses: Poster No.: Congress: Type: Authors: KeywordsDocumento8 páginasThe Benefit of Tru-Cut Biopsy in Breast Masses: Poster No.: Congress: Type: Authors: Keywordsم.محمدولدعليAinda não há avaliações
- The Role of Imaging in Cervical Cancer Staging - ESGOESTROESP Guidelines (Update 2023)Documento32 páginasThe Role of Imaging in Cervical Cancer Staging - ESGOESTROESP Guidelines (Update 2023)Limbert Rodríguez TiconaAinda não há avaliações
- Icru 82Documento67 páginasIcru 82Aditya DisdusAinda não há avaliações
- The Diagnostic Value of Ultrasound and Mammography in Detection of Breast Cancer in AlbaniaDocumento10 páginasThe Diagnostic Value of Ultrasound and Mammography in Detection of Breast Cancer in AlbaniaIJPHSAinda não há avaliações
- Laporan Indikator Kepatuhan Formularium 2020Documento26 páginasLaporan Indikator Kepatuhan Formularium 2020Erni Yessyca SimamoraAinda não há avaliações
- Clarification of Terminology in Medicati PDFDocumento12 páginasClarification of Terminology in Medicati PDFErni Yessyca SimamoraAinda não há avaliações
- Hubungan Kelengkapan Rekam Medis DGN Klaim Bpjs PDFDocumento7 páginasHubungan Kelengkapan Rekam Medis DGN Klaim Bpjs PDFErni Yessyca SimamoraAinda não há avaliações
- Antimicrobial Stewardship Program (Ri)Documento50 páginasAntimicrobial Stewardship Program (Ri)Erni Yessyca SimamoraAinda não há avaliações
- Aplikasi WISNDocumento9 páginasAplikasi WISNErni Yessyca SimamoraAinda não há avaliações
- Review Visi Dan Misi - Arief Wahyu SDocumento3 páginasReview Visi Dan Misi - Arief Wahyu SErni Yessyca SimamoraAinda não há avaliações
- Misi-Visi Rsup PersahabatanDocumento2 páginasMisi-Visi Rsup PersahabatanErni Yessyca SimamoraAinda não há avaliações
- Effects of Work Environment and Engagement On Nurses Organizational Commitment in Public Hospitals Lahore, PakistanDocumento6 páginasEffects of Work Environment and Engagement On Nurses Organizational Commitment in Public Hospitals Lahore, PakistanErni Yessyca SimamoraAinda não há avaliações
- ValidasiDocumento2 páginasValidasiErni Yessyca SimamoraAinda não há avaliações
- RWJF Collaboration PDFDocumento2 páginasRWJF Collaboration PDFErni Yessyca SimamoraAinda não há avaliações
- Pneumonia AspirasiDocumento7 páginasPneumonia AspirasiErni Yessyca SimamoraAinda não há avaliações
- Visi Dan Misi Rsud MatramanDocumento2 páginasVisi Dan Misi Rsud MatramanErni Yessyca SimamoraAinda não há avaliações
- HBP Moving-Ahead PDFDocumento2 páginasHBP Moving-Ahead PDFErni Yessyca SimamoraAinda não há avaliações
- Hepa-Merz: Hepatic EncephalopathyDocumento40 páginasHepa-Merz: Hepatic EncephalopathyErni Yessyca Simamora83% (6)
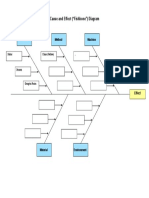
- Cause and Effect ("Fishbone") Diagram: Person Method MachineDocumento1 páginaCause and Effect ("Fishbone") Diagram: Person Method MachineErni Yessyca SimamoraAinda não há avaliações
- Meningitis TBDocumento11 páginasMeningitis TBErni Yessyca SimamoraAinda não há avaliações
- Jurnal DHF IndonesiaDocumento6 páginasJurnal DHF IndonesiaErni Yessyca SimamoraAinda não há avaliações
- 10 E-LibraryDocumento18 páginas10 E-LibraryErni Yessyca SimamoraAinda não há avaliações
- Meningitis TBDocumento11 páginasMeningitis TBErni Yessyca SimamoraAinda não há avaliações
- Study Group الملزمة الاولىDocumento233 páginasStudy Group الملزمة الاولىMoustafa MagdyAinda não há avaliações
- Respiratory MCQs LJDocumento7 páginasRespiratory MCQs LJfjghAinda não há avaliações
- Lesson 4Documento6 páginasLesson 4doldol ocampoAinda não há avaliações
- Assessment of Pregnant Woman 2023Documento2 páginasAssessment of Pregnant Woman 2023ysohidalgo13Ainda não há avaliações
- PATENTE - Worksheet - Nasogastric Tube Insertion, Feeding, and RemovalDocumento11 páginasPATENTE - Worksheet - Nasogastric Tube Insertion, Feeding, and RemovalSelwynVillamorPatenteAinda não há avaliações
- Airway Management and Common ConditionsDocumento34 páginasAirway Management and Common Conditionsrigo montejoAinda não há avaliações
- Cells and Organs of The Immune SystemDocumento53 páginasCells and Organs of The Immune SystemZyma EmaAinda não há avaliações
- Urinary Tract Infection (UTI) : Pharmacotherapeutics II YrDocumento20 páginasUrinary Tract Infection (UTI) : Pharmacotherapeutics II YrpawannnnAinda não há avaliações
- Evan's SyndromeDocumento94 páginasEvan's SyndromeKristine Joy Vivero BillonesAinda não há avaliações
- Obsessive Compulsive Disorder: Patient Treatment ManualDocumento20 páginasObsessive Compulsive Disorder: Patient Treatment ManualJay DraperAinda não há avaliações
- NZMSA Guide To Graduation 2012Documento40 páginasNZMSA Guide To Graduation 2012Vijaya RajAinda não há avaliações
- Toaz - Info Dispensing Incompatibilities and Adverse Drug Reactions Answer Key Red Pa PRDocumento17 páginasToaz - Info Dispensing Incompatibilities and Adverse Drug Reactions Answer Key Red Pa PRPRIYA SHEETAKAinda não há avaliações
- Pemeriksaan BMDDocumento43 páginasPemeriksaan BMDMisael ChristianAinda não há avaliações
- Pediatric Cardiac Arrest AlgorithmDocumento27 páginasPediatric Cardiac Arrest AlgorithmLinna AndrianiAinda não há avaliações
- Kuliah Hemoglobinopati - Uin Syarif Hidayatullah - Mei 2010Documento35 páginasKuliah Hemoglobinopati - Uin Syarif Hidayatullah - Mei 2010Nurraisya MutiyaniAinda não há avaliações
- (Ha Lab) Sas#9Documento9 páginas(Ha Lab) Sas#9Erwin RomeroAinda não há avaliações
- Final PhysicalDocumento409 páginasFinal PhysicalAbhishiktaAbhiAinda não há avaliações
- Alajar - Act9 - Biol 015Documento3 páginasAlajar - Act9 - Biol 015jarrettrayke14Ainda não há avaliações
- SBAR Communication Worksheet: SaferDocumento13 páginasSBAR Communication Worksheet: SaferBenny Riyan100% (1)
- Angina Pectoris: History TakingDocumento7 páginasAngina Pectoris: History TakingNavpreet KaurAinda não há avaliações
- Acute Respiratory IllnessDocumento18 páginasAcute Respiratory IllnessMobin Ur Rehman KhanAinda não há avaliações
- My Own Life: by Oliver SacksDocumento4 páginasMy Own Life: by Oliver SacksAmerigo VespucciAinda não há avaliações
- Reading - Age With Moderate DehydrationDocumento8 páginasReading - Age With Moderate DehydrationSophia IbuyanAinda não há avaliações
- Quiz TraumaDocumento1 páginaQuiz Traumaaqsa rehmanAinda não há avaliações
- Health Effects of Smoking Among Young PeopleDocumento2 páginasHealth Effects of Smoking Among Young PeopleJessicaAinda não há avaliações
- Viral InfectionsDocumento59 páginasViral InfectionsSajin AlexanderAinda não há avaliações
- Pa Tho Physiology of Diabetes InsipidusDocumento4 páginasPa Tho Physiology of Diabetes InsipidusteynsAinda não há avaliações
- Transplantation: Treatment Methods For Kidney FailureDocumento28 páginasTransplantation: Treatment Methods For Kidney FailurecopiimeiAinda não há avaliações
- Cardiac Glycosides 815Documento19 páginasCardiac Glycosides 815SanskritiAinda não há avaliações
- Internship Report Noor Arshad 28Documento80 páginasInternship Report Noor Arshad 28hammadAinda não há avaliações