Você também pode gostar
- Long-Term Outcomes in Patients Surviving Large Burns: The Musculoskeletal SystemDocumento12 páginasLong-Term Outcomes in Patients Surviving Large Burns: The Musculoskeletal SystemAlfin HidayatAinda não há avaliações
- Functioning of Stroke Survivors - A Validation of The ICF Core Set For Stroke in SwedenDocumento9 páginasFunctioning of Stroke Survivors - A Validation of The ICF Core Set For Stroke in SwedenMuhammadMusa47Ainda não há avaliações
- Elsherbiny 2017Documento8 páginasElsherbiny 2017Siti ChodijahAinda não há avaliações
- 1752 2897 4 7Documento7 páginas1752 2897 4 7ruba azfr-aliAinda não há avaliações
- 36 Using Quality Oflife Measurements in Pharmacoepidemiology ResearchDocumento11 páginas36 Using Quality Oflife Measurements in Pharmacoepidemiology Researchfarmasiums15Ainda não há avaliações
- Core Outomes Set ESJ2015Documento16 páginasCore Outomes Set ESJ2015Ju ChangAinda não há avaliações
- Costs-Efectiveness Interventions Review, Wortman 2018Documento23 páginasCosts-Efectiveness Interventions Review, Wortman 2018Zuemy BatunAinda não há avaliações
- ACV 2 CIF Paanalahti2013Documento10 páginasACV 2 CIF Paanalahti2013Fabian SepulvedaAinda não há avaliações
- Long Term Outcome of Functional Independence and Quality of Life After Traumatic SCI in GermanyDocumento8 páginasLong Term Outcome of Functional Independence and Quality of Life After Traumatic SCI in GermanyLuis Diego Verastegui LeguaAinda não há avaliações
- Pressure Ulcer QoLDocumento5 páginasPressure Ulcer QoLSevalAinda não há avaliações
- The General Health Questionnaire-28 (GHQ-28) As An Outcome Measurement in A Randomized Controlled Trial in A Norwegian Stroke PopulationDocumento11 páginasThe General Health Questionnaire-28 (GHQ-28) As An Outcome Measurement in A Randomized Controlled Trial in A Norwegian Stroke PopulationAV GaneshAinda não há avaliações
- Grossman Mindfulness MA Psychosom Res 2004Documento10 páginasGrossman Mindfulness MA Psychosom Res 2004Kamilou Kamilos ValiaAinda não há avaliações
- Prognosis of Six-Month Functioning After Moderate To Severe Traumatic Brain Injury: A Systematic Review of Prospective Cohort StudiesDocumento12 páginasPrognosis of Six-Month Functioning After Moderate To Severe Traumatic Brain Injury: A Systematic Review of Prospective Cohort StudiesYan Sheng HoAinda não há avaliações
- RATetal IntJClinEpidemio2005Documento10 páginasRATetal IntJClinEpidemio2005BRAIN SHARPNERAinda não há avaliações
- Karcioglu 2018Documento8 páginasKarcioglu 2018Liana HarnumAinda não há avaliações
- Goldberg's General Health Questionnaire: Tidsskrift For Den Norske Legeforening June 1989Documento11 páginasGoldberg's General Health Questionnaire: Tidsskrift For Den Norske Legeforening June 1989w dAinda não há avaliações
- A Systematic Review of Treatments For Mild Traumatic Brain InjuryDocumento3 páginasA Systematic Review of Treatments For Mild Traumatic Brain InjurySergio Machado NeurocientistaAinda não há avaliações
- Articulo 4 Sesión 1 Visión General Reed Et Al 2018Documento10 páginasArticulo 4 Sesión 1 Visión General Reed Et Al 2018manuel ñiqueAinda não há avaliações
- 10 1111@jep 13190Documento10 páginas10 1111@jep 13190carlosso16hotmail.comAinda não há avaliações
- Outcome Metrics After Bur N Injury: From Patient-Reported Outcome Measures To Value-Based Health CareDocumento4 páginasOutcome Metrics After Bur N Injury: From Patient-Reported Outcome Measures To Value-Based Health CareJoao FonsecaAinda não há avaliações
- Bab 2Documento2 páginasBab 2SANDA NABILAH FATINAinda não há avaliações
- The Validity and Reliability of The Healthy LifestDocumento13 páginasThe Validity and Reliability of The Healthy LifestMantraDebosaAinda não há avaliações
- Antipsychotic Treatment A Systematic Literature Review and Meta Analysis of Qualitative StudiesDocumento12 páginasAntipsychotic Treatment A Systematic Literature Review and Meta Analysis of Qualitative StudiesmafeAinda não há avaliações
- Paper 4Documento13 páginasPaper 4Pablo Cuevas SaldivarAinda não há avaliações
- Domenesio (2021) Client Experiences With Holistic Neuropsychological Rehabilitation It Is An Ongoing ProcessDocumento24 páginasDomenesio (2021) Client Experiences With Holistic Neuropsychological Rehabilitation It Is An Ongoing Processhoranvera10Ainda não há avaliações
- AC Joint InjuryDocumento13 páginasAC Joint InjuryFarhan JustisiaAinda não há avaliações
- Moyer 2001Documento15 páginasMoyer 2001Duglas Liam Quintanilla VelazcoAinda não há avaliações
- Manual Therapy: Original ArticleDocumento6 páginasManual Therapy: Original Articleubiktrash1492Ainda não há avaliações
- Original ArticlesDocumento7 páginasOriginal ArticlesĐan TâmAinda não há avaliações
- Manipulação e Mobilização para o Tratamento Da Dor Crônica Inespecífica Do Pescoço Uma Revisão Sistemática e Meta-Análise para Um Painel de AdequaçãoDocumento24 páginasManipulação e Mobilização para o Tratamento Da Dor Crônica Inespecífica Do Pescoço Uma Revisão Sistemática e Meta-Análise para Um Painel de AdequaçãoCelso SouzaAinda não há avaliações
- Original Report: J Rehabil Med 45Documento12 páginasOriginal Report: J Rehabil Med 45Novia RambakAinda não há avaliações
- Pone 0204774Documento52 páginasPone 0204774Karina OktaviyadiAinda não há avaliações
- Pain Management - A Decade's Perspective of A New SubspecialtyDocumento8 páginasPain Management - A Decade's Perspective of A New SubspecialtyDavid PrivatAinda não há avaliações
- Quality of Life Tools in Head and Neck OncologyDocumento15 páginasQuality of Life Tools in Head and Neck OncologyAnonymous 9UQNN0Ainda não há avaliações
- Best Practices For Elderly Hip Fracture Patients. A Systematic Overview of The Evidence.Documento7 páginasBest Practices For Elderly Hip Fracture Patients. A Systematic Overview of The Evidence.Tuấn Lê (jose)Ainda não há avaliações
- Similarities and Differences Between Evaluation Protocols in Physical Therapy and Occupational Therapy - A Case StudyDocumento5 páginasSimilarities and Differences Between Evaluation Protocols in Physical Therapy and Occupational Therapy - A Case Studyshiela marie danielAinda não há avaliações
- Mindfulness meditation improves mental and physical healthDocumento10 páginasMindfulness meditation improves mental and physical healthGABRIELAinda não há avaliações
- A Randomised Comparison of Cognitive Behavioural Therapy CBT and Eye Movement Desensitisation and Reprocessing EMDR in Disaster Exposed ChildrenDocumento12 páginasA Randomised Comparison of Cognitive Behavioural Therapy CBT and Eye Movement Desensitisation and Reprocessing EMDR in Disaster Exposed ChildrenWaleska ZomosaAinda não há avaliações
- Artigo Mobilização PrecoceDocumento9 páginasArtigo Mobilização PrecoceLuciana AlexandreAinda não há avaliações
- A Short Questionnaire For The Assessment of Quality of Life in Patients With Chronic Obstructive Pulmonary Disease: Psychometric Properties of VQ11Documento11 páginasA Short Questionnaire For The Assessment of Quality of Life in Patients With Chronic Obstructive Pulmonary Disease: Psychometric Properties of VQ11elonaAinda não há avaliações
- Pain Assessment Tools For Older Adults With Dementia in Long-Term Care Facilities: A Systematic ReviewDocumento14 páginasPain Assessment Tools For Older Adults With Dementia in Long-Term Care Facilities: A Systematic Review12099964Ainda não há avaliações
- Medi 100 E25963Documento4 páginasMedi 100 E25963LUIS AYALAAinda não há avaliações
- Stroke Scales and Trajectory of Recovery A Major Concern For Patients and Nurses AlikeDocumento7 páginasStroke Scales and Trajectory of Recovery A Major Concern For Patients and Nurses AlikeAnonymous XO9RqHhOgiAinda não há avaliações
- (2017) IBD - Spesific Health Related QoL InstrumentDocumento13 páginas(2017) IBD - Spesific Health Related QoL InstrumentfikriafisAinda não há avaliações
- Developing Clinical Guidelines for Initial Trauma Patient AssessmentDocumento3 páginasDeveloping Clinical Guidelines for Initial Trauma Patient AssessmentErikaCacatianAinda não há avaliações
- Anaesthesia - 2018 - Gerth - Changes in Health Related Quality of Life After Discharge From An Intensive Care Unit ADocumento9 páginasAnaesthesia - 2018 - Gerth - Changes in Health Related Quality of Life After Discharge From An Intensive Care Unit ANut SamprasitAinda não há avaliações
- Mental Health Inventory: Sensitivity and Specificity of The Portuguese Version of The MHI-38 and MHI-5Documento18 páginasMental Health Inventory: Sensitivity and Specificity of The Portuguese Version of The MHI-38 and MHI-5Thao CaoAinda não há avaliações
- Pincus 2006Documento9 páginasPincus 2006Claudio Andrés Olmos de AguileraAinda não há avaliações
- Antipsychotic Treatment - A Systematic Literature Review and Meta-Analysis of Qualitative StudiesDocumento12 páginasAntipsychotic Treatment - A Systematic Literature Review and Meta-Analysis of Qualitative StudiesPriti BhosleAinda não há avaliações
- Aarstad 2017Documento11 páginasAarstad 2017Andressa A.Ainda não há avaliações
- Intensive Insulin Therapy in Intensive Care: An Example of The Struggle To Implement Evidence-Based MedicineDocumento6 páginasIntensive Insulin Therapy in Intensive Care: An Example of The Struggle To Implement Evidence-Based MedicineAnnisa MaharaniAinda não há avaliações
- Caregiver-Mediated Exercises With E-Health Support For Early Supported Discharge After Stroke (CARE4STROKE) : A Randomized Controlled TrialDocumento15 páginasCaregiver-Mediated Exercises With E-Health Support For Early Supported Discharge After Stroke (CARE4STROKE) : A Randomized Controlled TrialyenrilisnaAinda não há avaliações
- Aichner 2002Documento15 páginasAichner 2002cah bagusAinda não há avaliações
- 1 s2.0 S1201971214017214 Main PDFDocumento5 páginas1 s2.0 S1201971214017214 Main PDFYohanna ekasntAinda não há avaliações
- Manual Therapy: Systematic ReviewDocumento8 páginasManual Therapy: Systematic Reviewubiktrash1492Ainda não há avaliações
- Van KesselDocumento9 páginasVan KesselJorge Fernández BaluarteAinda não há avaliações
- Emergency Department Triage Scales and Their Components: A Systematic Review of The Scientific EvidenceDocumento13 páginasEmergency Department Triage Scales and Their Components: A Systematic Review of The Scientific Evidencearofah hAinda não há avaliações
- Document PDFDocumento13 páginasDocument PDFMuizhima MuizAinda não há avaliações
- Stroke Article 1Documento10 páginasStroke Article 1api-292843843Ainda não há avaliações
- Aaam Face Thread c5 2019 FlyerDocumento1 páginaAaam Face Thread c5 2019 FlyerTina HerreraAinda não há avaliações
- Clinical Pathway for Inguinal Hernia RepairDocumento6 páginasClinical Pathway for Inguinal Hernia RepairTina HerreraAinda não há avaliações
- Clinical Pathway Limphadenopaty ColiDocumento6 páginasClinical Pathway Limphadenopaty ColiTina HerreraAinda não há avaliações
- 167 FullDocumento5 páginas167 FullTina HerreraAinda não há avaliações
- CP AppendectomyDocumento6 páginasCP AppendectomyTina HerreraAinda não há avaliações
- Tumor Immune Escape Mechanisms: Yi Ting Koh,, M. Luz García-Hernández,, and W. Martin KastDocumento26 páginasTumor Immune Escape Mechanisms: Yi Ting Koh,, M. Luz García-Hernández,, and W. Martin KastTina HerreraAinda não há avaliações
- Pie 2018Documento5 páginasPie 2018Tina HerreraAinda não há avaliações
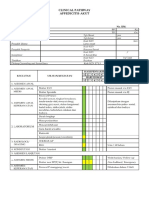
- Clinical Pathway Apendisitis AcutaDocumento7 páginasClinical Pathway Apendisitis AcutaTina HerreraAinda não há avaliações
- Aaam Face Thread c5 2019 FlyerDocumento1 páginaAaam Face Thread c5 2019 FlyerTina HerreraAinda não há avaliações
- Controversy in Head Injury, Abdul Hafid PDFDocumento31 páginasControversy in Head Injury, Abdul Hafid PDFTina HerreraAinda não há avaliações
- Comparing Propranolol and Corticosteroids for Pediatric HemangiomasDocumento9 páginasComparing Propranolol and Corticosteroids for Pediatric HemangiomasTina HerreraAinda não há avaliações
- Comparing Propranolol and Corticosteroids for Pediatric HemangiomasDocumento9 páginasComparing Propranolol and Corticosteroids for Pediatric HemangiomasTina HerreraAinda não há avaliações
- Guia de Bologna-2013Documento14 páginasGuia de Bologna-2013andreigustvAinda não há avaliações
- Intracranial Pathophysiology, Zainal MDocumento25 páginasIntracranial Pathophysiology, Zainal MTina HerreraAinda não há avaliações
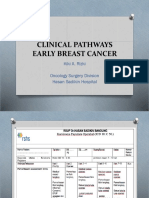
- CP Early Breast CancerDocumento8 páginasCP Early Breast CancerTina HerreraAinda não há avaliações
- Controversy in Head Injury, Abdul Hafid PDFDocumento31 páginasControversy in Head Injury, Abdul Hafid PDFTina HerreraAinda não há avaliações
- Pre-Hospital Severe Traumatic Brain Injury - Comparison of Outcome in Paramedic Versus Physician Staffed Emergency Medical Services (2016)Documento7 páginasPre-Hospital Severe Traumatic Brain Injury - Comparison of Outcome in Paramedic Versus Physician Staffed Emergency Medical Services (2016)Tina HerreraAinda não há avaliações
- Biomolecular and Immunological, Sofia MDocumento64 páginasBiomolecular and Immunological, Sofia MTina HerreraAinda não há avaliações
- Brain Protection, M.Ramli PDFDocumento50 páginasBrain Protection, M.Ramli PDFTina HerreraAinda não há avaliações
- National Guideline, Peter LDocumento51 páginasNational Guideline, Peter LTina HerreraAinda não há avaliações
- Thoracic Lumbar, Eko AgusDocumento32 páginasThoracic Lumbar, Eko AgusTina HerreraAinda não há avaliações
- Biomelecular Aspect, Irawan YusufDocumento23 páginasBiomelecular Aspect, Irawan YusufTina HerreraAinda não há avaliações
- Brain Protection, M.Ramli PDFDocumento50 páginasBrain Protection, M.Ramli PDFTina HerreraAinda não há avaliações
- Pharmacotherapy of Traumatic Brain Injury (2015)Documento6 páginasPharmacotherapy of Traumatic Brain Injury (2015)Tina HerreraAinda não há avaliações
- Brain Protection, M.Ramli PDFDocumento50 páginasBrain Protection, M.Ramli PDFTina HerreraAinda não há avaliações
- Outcome of Surgically Treated Traumatic Extradural Hematoma (2016)Documento9 páginasOutcome of Surgically Treated Traumatic Extradural Hematoma (2016)Tina HerreraAinda não há avaliações
- Soal Ujian NeurotraumaDocumento22 páginasSoal Ujian NeurotraumaTina HerreraAinda não há avaliações
- Jurnal NCDocumento12 páginasJurnal NCTina HerreraAinda não há avaliações
- SarcasmDocumento6 páginasSarcasmMarto FeAinda não há avaliações
- EPT Reviewer - Reading ComprehensionDocumento4 páginasEPT Reviewer - Reading ComprehensionLuther Gersin CañaAinda não há avaliações
- Final MBBS Part I Lectures Vol I PDFDocumento82 páginasFinal MBBS Part I Lectures Vol I PDFHan TunAinda não há avaliações
- WillisTodorov (2006) Cognitive BiasDocumento7 páginasWillisTodorov (2006) Cognitive BiasrogertitleAinda não há avaliações
- Jude Anthony Beato Fabellare: ObjectiveDocumento3 páginasJude Anthony Beato Fabellare: ObjectiveJude FabellareAinda não há avaliações
- FST 430 Innovation and Food Product Development Syllabus Spring 2014 10 30 2013Documento7 páginasFST 430 Innovation and Food Product Development Syllabus Spring 2014 10 30 2013Ann Myril Chua TiuAinda não há avaliações
- Purposive AssignmentDocumento3 páginasPurposive AssignmentJune Clear Olivar LlabanAinda não há avaliações
- Minitab Survey Analysis With ANOVA and MoreDocumento4 páginasMinitab Survey Analysis With ANOVA and MoreAdnan MustafićAinda não há avaliações
- The Veldt by Ray Bradbury: JavierDocumento5 páginasThe Veldt by Ray Bradbury: Javierapi-334247362Ainda não há avaliações
- Emotions and how to communicate feelingsDocumento8 páginasEmotions and how to communicate feelingsnurulwaznahAinda não há avaliações
- The Concept of Powerlessness in Patient Treatment Nursing EssayDocumento38 páginasThe Concept of Powerlessness in Patient Treatment Nursing EssayreginesulibAinda não há avaliações
- 17 Tips Taking Initiative at WorkDocumento16 páginas17 Tips Taking Initiative at WorkHarshraj Salvitthal100% (1)
- Your Honor, We Would Like To Have This Psychological Assessment Marked As P-10Documento7 páginasYour Honor, We Would Like To Have This Psychological Assessment Marked As P-10Claudine ArrabisAinda não há avaliações
- Attachment StyleDocumento14 páginasAttachment StylewidyaAinda não há avaliações
- If How Tos Were EnoughDocumento57 páginasIf How Tos Were Enoughapi-3745547Ainda não há avaliações
- Project Based LearningDocumento1 páginaProject Based Learningapi-311318294Ainda não há avaliações
- AMORC What Constitutes A High Degree Member in AMORC 2Documento3 páginasAMORC What Constitutes A High Degree Member in AMORC 2Francis EjikeAinda não há avaliações
- Modul Q Gradder Class PDFDocumento446 páginasModul Q Gradder Class PDFbudimanheryantoAinda não há avaliações
- Guanavante GeniusDocumento270 páginasGuanavante Geniusartisanicview100% (3)
- Edward T. Hall - Beyond Culture-Doubleday (1976)Documento384 páginasEdward T. Hall - Beyond Culture-Doubleday (1976)Tristan ZarateAinda não há avaliações
- Mental Stress Evaluation Using Heart Rate Variability AnalysisDocumento7 páginasMental Stress Evaluation Using Heart Rate Variability AnalysisKalpeshPatilAinda não há avaliações
- Open Research Online: Kinky Clients, Kinky Counselling? The Challenges and Potentials of BDSMDocumento37 páginasOpen Research Online: Kinky Clients, Kinky Counselling? The Challenges and Potentials of BDSMmonica cozarevAinda não há avaliações
- Benchmarking Clubs: A Guide For Small and Diaspora NgosDocumento7 páginasBenchmarking Clubs: A Guide For Small and Diaspora NgosEngMohamedReyadHelesyAinda não há avaliações
- XII Project Work on Gandhi's LifeDocumento4 páginasXII Project Work on Gandhi's Liferandom idAinda não há avaliações
- Translation Methods 8Documento3 páginasTranslation Methods 8Mădălina TodincaAinda não há avaliações
- Freshmen Seminar Syllabus 2017-28Documento4 páginasFreshmen Seminar Syllabus 2017-28api-296097282Ainda não há avaliações
- A Study On Job Satisfaction With Regard To Electrical PointDocumento9 páginasA Study On Job Satisfaction With Regard To Electrical PointMohammed AfnanAinda não há avaliações
- Sentence WritingDocumento2 páginasSentence WritingLee Mei Chai李美齊Ainda não há avaliações
- Ecosoc Chair ReportDocumento9 páginasEcosoc Chair Reportapi-408542393Ainda não há avaliações
- Lesson 9 - The Spiritual SelfDocumento1 páginaLesson 9 - The Spiritual SelfmichelleAinda não há avaliações
- Weapons of Mass Instruction: A Schoolteacher's Journey Through the Dark World of Compulsory SchoolingNo EverandWeapons of Mass Instruction: A Schoolteacher's Journey Through the Dark World of Compulsory SchoolingNota: 4.5 de 5 estrelas4.5/5 (149)
- Summary: The 5AM Club: Own Your Morning. Elevate Your Life. by Robin Sharma: Key Takeaways, Summary & AnalysisNo EverandSummary: The 5AM Club: Own Your Morning. Elevate Your Life. by Robin Sharma: Key Takeaways, Summary & AnalysisNota: 4.5 de 5 estrelas4.5/5 (22)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipNo EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipNota: 4.5 de 5 estrelas4.5/5 (1135)
- The 16 Undeniable Laws of Communication: Apply Them and Make the Most of Your MessageNo EverandThe 16 Undeniable Laws of Communication: Apply Them and Make the Most of Your MessageNota: 5 de 5 estrelas5/5 (72)
- Summary: Greenlights: by Matthew McConaughey: Key Takeaways, Summary & AnalysisNo EverandSummary: Greenlights: by Matthew McConaughey: Key Takeaways, Summary & AnalysisNota: 4 de 5 estrelas4/5 (6)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisNo EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisNota: 5 de 5 estrelas5/5 (3)
- Summary: I'm Glad My Mom Died: by Jennette McCurdy: Key Takeaways, Summary & AnalysisNo EverandSummary: I'm Glad My Mom Died: by Jennette McCurdy: Key Takeaways, Summary & AnalysisNota: 4.5 de 5 estrelas4.5/5 (2)
- Summary: The Laws of Human Nature: by Robert Greene: Key Takeaways, Summary & AnalysisNo EverandSummary: The Laws of Human Nature: by Robert Greene: Key Takeaways, Summary & AnalysisNota: 4.5 de 5 estrelas4.5/5 (30)
- Grit: The Power of Passion and PerseveranceNo EverandGrit: The Power of Passion and PerseveranceNota: 4.5 de 5 estrelas4.5/5 (1872)
- Dumbing Us Down: The Hidden Curriculum of Compulsory SchoolingNo EverandDumbing Us Down: The Hidden Curriculum of Compulsory SchoolingNota: 4.5 de 5 estrelas4.5/5 (495)
- Make It Stick by Peter C. Brown, Henry L. Roediger III, Mark A. McDaniel - Book Summary: The Science of Successful LearningNo EverandMake It Stick by Peter C. Brown, Henry L. Roediger III, Mark A. McDaniel - Book Summary: The Science of Successful LearningNota: 4.5 de 5 estrelas4.5/5 (55)
- Financial Feminist: Overcome the Patriarchy's Bullsh*t to Master Your Money and Build a Life You LoveNo EverandFinancial Feminist: Overcome the Patriarchy's Bullsh*t to Master Your Money and Build a Life You LoveNota: 5 de 5 estrelas5/5 (1)
- Summary: Trading in the Zone: Trading in the Zone: Master the Market with Confidence, Discipline, and a Winning Attitude by Mark Douglas: Key Takeaways, Summary & AnalysisNo EverandSummary: Trading in the Zone: Trading in the Zone: Master the Market with Confidence, Discipline, and a Winning Attitude by Mark Douglas: Key Takeaways, Summary & AnalysisNota: 5 de 5 estrelas5/5 (15)
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindNo EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindNota: 4.5 de 5 estrelas4.5/5 (1)
- Follow The Leader: A Collection Of The Best Lectures On LeadershipNo EverandFollow The Leader: A Collection Of The Best Lectures On LeadershipNota: 5 de 5 estrelas5/5 (122)
- Little Soldiers: An American Boy, a Chinese School, and the Global Race to AchieveNo EverandLittle Soldiers: An American Boy, a Chinese School, and the Global Race to AchieveNota: 4 de 5 estrelas4/5 (25)
- How to Improve English Speaking: How to Become a Confident and Fluent English SpeakerNo EverandHow to Improve English Speaking: How to Become a Confident and Fluent English SpeakerNota: 4.5 de 5 estrelas4.5/5 (56)
- Think Ahead: 7 Decisions You Can Make Today for the God-Honoring Life You Want TomorrowNo EverandThink Ahead: 7 Decisions You Can Make Today for the God-Honoring Life You Want TomorrowNota: 5 de 5 estrelas5/5 (7)
- Whatever It Takes: Geoffrey Canada's Quest to Change Harlem and AmericaNo EverandWhatever It Takes: Geoffrey Canada's Quest to Change Harlem and AmericaNota: 4 de 5 estrelas4/5 (79)
- Summary of The Power of Habit: Why We Do What We Do in Life and Business by Charles DuhiggNo EverandSummary of The Power of Habit: Why We Do What We Do in Life and Business by Charles DuhiggNota: 4.5 de 5 estrelas4.5/5 (261)
- Weapons of Mass Instruction: A Schoolteacher's Journey Through the Dark World of Compulsory SchoolingNo EverandWeapons of Mass Instruction: A Schoolteacher's Journey Through the Dark World of Compulsory SchoolingNota: 4 de 5 estrelas4/5 (59)