Você também pode gostar
- Cell Phones and Brain Cancer: Unlocking The Controversy?Documento21 páginasCell Phones and Brain Cancer: Unlocking The Controversy?maniAinda não há avaliações
- Morning case: CH. Nguyễn Xuân PhongDocumento47 páginasMorning case: CH. Nguyễn Xuân PhongQuynh TranAinda não há avaliações
- Rabies and Its Preventive Management: DR M Amir Sohail MBBS DCHDocumento59 páginasRabies and Its Preventive Management: DR M Amir Sohail MBBS DCHdrmasAinda não há avaliações
- Bengin SGT 2023Documento11 páginasBengin SGT 2023Hazem MouradAinda não há avaliações
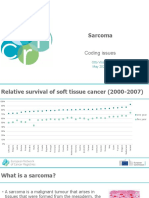
- ENCR2021 S4 SarcomaDocumento28 páginasENCR2021 S4 SarcomaFernando SilalahiAinda não há avaliações
- Salivary Gland TumorDocumento67 páginasSalivary Gland TumorMeri NovitaAinda não há avaliações
- Epithelial Tumours - SreejaDocumento184 páginasEpithelial Tumours - SreejaaakiAinda não há avaliações
- Cytogenetics - Lesson 1Documento24 páginasCytogenetics - Lesson 1Angelina AquinoAinda não há avaliações
- Oral Neoplasma III SoundDocumento53 páginasOral Neoplasma III SoundJi ChuAinda não há avaliações
- Head and Neck Mucosal MelanomaDocumento5 páginasHead and Neck Mucosal MelanomaHAMIDAinda não há avaliações
- Update On Current Problems in Colorectal Liver MetastasisDocumento49 páginasUpdate On Current Problems in Colorectal Liver MetastasisabiramirajalaksmiAinda não há avaliações
- L4. Viral Vectors - StudentDocumento26 páginasL4. Viral Vectors - Studentstaoge062028100% (1)
- Salivary Gland Tumors GuideDocumento25 páginasSalivary Gland Tumors GuidedrpnnreddyAinda não há avaliações
- Breast Cancer UG Lecture 1Documento60 páginasBreast Cancer UG Lecture 1Ribhav GuptaAinda não há avaliações
- Nervo US Syste M: Endocrine SystemDocumento2 páginasNervo US Syste M: Endocrine SystemEric A Colinares Jr.Ainda não há avaliações
- Thurs3 Spinal Tumors Molnar Updated1.9.19Documento12 páginasThurs3 Spinal Tumors Molnar Updated1.9.19Ikon ikonicAinda não há avaliações
- Oncology Nursing (Word) Bulleted For NSG RevieweesDocumento8 páginasOncology Nursing (Word) Bulleted For NSG Revieweesswitlipz100% (1)
- SEMINAR OMFS BDSDocumento17 páginasSEMINAR OMFS BDSHarshal AbdullaAinda não há avaliações
- 2 Nasopharyngeal Dise (Sept. 2019) - StudentDocumento80 páginas2 Nasopharyngeal Dise (Sept. 2019) - StudentNicAinda não há avaliações
- Evaluation and Management of Neck MassesDocumento38 páginasEvaluation and Management of Neck MassesShaxawan Mahmood AliAinda não há avaliações
- NEOPLASMA (1Documento65 páginasNEOPLASMA (1Syeila marselaAinda não há avaliações
- Malignant Tumors of The Facial SkinDocumento78 páginasMalignant Tumors of The Facial SkinMladen PazinAinda não há avaliações
- Epidemiology of CancerDocumento21 páginasEpidemiology of Cancerhussain AltaherAinda não há avaliações
- Multiple Endocrine NeoplasiaDocumento4 páginasMultiple Endocrine NeoplasiaDivya RanasariaAinda não há avaliações
- Studying Health and Health Care: Manitoba Centre For Health PolicyDocumento29 páginasStudying Health and Health Care: Manitoba Centre For Health Policyaijaz1inAinda não há avaliações
- Shibini Seminar Omfs (19)Documento17 páginasShibini Seminar Omfs (19)Harshal AbdullaAinda não há avaliações
- Salivary GlandsDocumento58 páginasSalivary GlandsApollo DentalAinda não há avaliações
- Cytogenetics: Prepared By: Arlene T. Conag, RMT, LPT InstructorDocumento107 páginasCytogenetics: Prepared By: Arlene T. Conag, RMT, LPT InstructorAngelina AquinoAinda não há avaliações
- PA - Dasar Neoplasma (DrBerti) PDFDocumento67 páginasPA - Dasar Neoplasma (DrBerti) PDFElearning FK UnhasAinda não há avaliações
- 26.salivary SlandsDocumento8 páginas26.salivary SlandsDurga VoraAinda não há avaliações
- Tumors of The Jaw and Oral MucosaDocumento18 páginasTumors of The Jaw and Oral MucosaDaniela LeonteAinda não há avaliações
- Diabetic Neph Ropa ThyDocumento90 páginasDiabetic Neph Ropa ThySandra Zarate GonzalesAinda não há avaliações
- Review of Cancer Types, Diagnosis, TreatmentDocumento54 páginasReview of Cancer Types, Diagnosis, TreatmentAbdul Hamid Al FarsiAinda não há avaliações
- (Fig. 17.3, A) : 3. Adenoma-Carcinoma Sequence Evolves From Pre-Existing Adenomas, Referred To AsDocumento31 páginas(Fig. 17.3, A) : 3. Adenoma-Carcinoma Sequence Evolves From Pre-Existing Adenomas, Referred To AsdystoAinda não há avaliações
- Understanding Eye Tumors and Skin CancersDocumento53 páginasUnderstanding Eye Tumors and Skin CancersAzilu FalaAinda não há avaliações
- Renal TransplantationDocumento57 páginasRenal Transplantationapi-376028367% (3)
- Paranasal Sinus Tumours ManagementDocumento69 páginasParanasal Sinus Tumours ManagementSACHIN SAinda não há avaliações
- Salivary Gland Neoplasm: Dr. Saad Al-Muhayawi. M.D., FRCSC Associate Professor & Consultant ORL Head & Neck SurgeryDocumento43 páginasSalivary Gland Neoplasm: Dr. Saad Al-Muhayawi. M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgeryraishern5475Ainda não há avaliações
- Kuliah Kelainan KulitDocumento47 páginasKuliah Kelainan KulitdinahzrAinda não há avaliações
- Soft Tissue and Bone Tumor Types and CharacteristicsDocumento92 páginasSoft Tissue and Bone Tumor Types and CharacteristicsItsirch AydinAinda não há avaliações
- TMP C814Documento51 páginasTMP C814Frontiers100% (1)
- Curr Diag Pathol-2006-12 - Sinonasal CarcinomasDocumento14 páginasCurr Diag Pathol-2006-12 - Sinonasal Carcinomasdarmayanti ibnuAinda não há avaliações
- Colon Polyp Types, Causes, Diagnosis and TreatmentDocumento30 páginasColon Polyp Types, Causes, Diagnosis and TreatmentIndhumathiAinda não há avaliações
- Neuro-Onkologi: Bagian/SMF Saraf FK-UGM/RS Dr. Sardjito YogyakartaDocumento59 páginasNeuro-Onkologi: Bagian/SMF Saraf FK-UGM/RS Dr. Sardjito YogyakartaNovasiska Indriyani HutajuluAinda não há avaliações
- Radiation Therapy Treatment Planning and Post-Care GuideDocumento93 páginasRadiation Therapy Treatment Planning and Post-Care GuideVyomaAinda não há avaliações
- Cellular Aberrations NotesDocumento22 páginasCellular Aberrations NotesH50% (2)
- Oral Neoplasma IDocumento31 páginasOral Neoplasma INandika 'ndek' DewaraAinda não há avaliações
- Oncology Pathology Tanuvas NotesDocumento17 páginasOncology Pathology Tanuvas NotesNagesh NAinda não há avaliações
- skinL5-WEB09Documento41 páginasskinL5-WEB09Gwyneth Koleen LopezAinda não há avaliações
- Principles of Neoplasia (New)Documento125 páginasPrinciples of Neoplasia (New)egyfellowpathologyAinda não há avaliações
- SEO-Optimized Title for Neoplasia DocumentTITLEDocumento61 páginasSEO-Optimized Title for Neoplasia DocumentTITLEOsama SaidatAinda não há avaliações
- UVEITIS ESSENTIALSeditDocumento38 páginasUVEITIS ESSENTIALSeditSatria WidyatamaAinda não há avaliações
- Onco - Day 1 Final SVDocumento170 páginasOnco - Day 1 Final SVApril Mae Magos LabradorAinda não há avaliações
- Institute of Medicine (IOM) Committee To Review Adverse Effects of Vaccines January 2010, National Academies of Sciences, Engineering, and MedicineDocumento4 páginasInstitute of Medicine (IOM) Committee To Review Adverse Effects of Vaccines January 2010, National Academies of Sciences, Engineering, and MedicineCitizen WellsAinda não há avaliações
- Basic Concepts of Cancer: Mohamad Bayu SahadewaDocumento34 páginasBasic Concepts of Cancer: Mohamad Bayu SahadewaHendra EfendiAinda não há avaliações
- NeoplasiaDocumento45 páginasNeoplasiaQanita RehmanAinda não há avaliações
- Kapita Selekta Onkologi THTDocumento46 páginasKapita Selekta Onkologi THTPutri Dwi KartiniAinda não há avaliações
- Salivaryglandtumors 150912063235 Lva1 App6892Documento213 páginasSalivaryglandtumors 150912063235 Lva1 App6892Waqas IqbalAinda não há avaliações
- EANM Lymphoscintigraphy GuidelinesDocumento17 páginasEANM Lymphoscintigraphy Guidelinesayodeji78Ainda não há avaliações
- Guideline VentilationperfusionDocumento15 páginasGuideline Ventilationperfusionvani marindaniAinda não há avaliações
- NEN2009090002184Documento6 páginasNEN2009090002184Mario MutuleanuAinda não há avaliações
- ESMO Epidemiology Classification and Clinical Presentation of NETs A European - Perspective PDFDocumento39 páginasESMO Epidemiology Classification and Clinical Presentation of NETs A European - Perspective PDFMario MutuleanuAinda não há avaliações
- 2015 EANM Lymphoscin SentinelNodeDocumento17 páginas2015 EANM Lymphoscin SentinelNodeMario MutuleanuAinda não há avaliações
- Essentials of Nuclear Medicine Imaging 6thDocumento611 páginasEssentials of Nuclear Medicine Imaging 6thayodeji78Ainda não há avaliações
- ESMO Epidemiology Classification and Clinical Presentation of NETs A European - Perspective PDFDocumento39 páginasESMO Epidemiology Classification and Clinical Presentation of NETs A European - Perspective PDFMario MutuleanuAinda não há avaliações
- Curs de Gastro - MOTILITATEDocumento49 páginasCurs de Gastro - MOTILITATEMădălina RădulescuAinda não há avaliações
- Treatment of Class II MalocclusionsDocumento148 páginasTreatment of Class II MalocclusionsRenu Ann Mathew100% (2)
- Thomas Rakosi CefalometrieDocumento224 páginasThomas Rakosi CefalometrieMario Mutuleanu100% (7)
- ENETS Consensus Guidelines For The Standards of Care in Neuroendocrine Tumors: Biochemical MarkersDocumento9 páginasENETS Consensus Guidelines For The Standards of Care in Neuroendocrine Tumors: Biochemical MarkersMario MutuleanuAinda não há avaliações
- Varicella Self DeclarationDocumento1 páginaVaricella Self DeclarationMario MutuleanuAinda não há avaliações
- Opioids Renal Hepatic DysfunctionDocumento9 páginasOpioids Renal Hepatic DysfunctionMadalina PopescuAinda não há avaliações
- Orthodontic Extrusion: Periodontal Considerations and ApplicationsDocumento6 páginasOrthodontic Extrusion: Periodontal Considerations and ApplicationsMario MutuleanuAinda não há avaliações
- Circulation 2006 May 113 (20) 2454-61Documento1 páginaCirculation 2006 May 113 (20) 2454-61Mario MutuleanuAinda não há avaliações
- Biocel Sub Rezolvate 2009Documento25 páginasBiocel Sub Rezolvate 2009ariadna89100% (2)
- Cardiology2 110608163006 Phpapp02Documento118 páginasCardiology2 110608163006 Phpapp02Mario MutuleanuAinda não há avaliações
- Development of the MandibleDocumento9 páginasDevelopment of the MandibleHub SciAinda não há avaliações
- Hem - Lab 4 Retic - 09Documento9 páginasHem - Lab 4 Retic - 09djebrutAinda não há avaliações
- Suggested Answers To Exercise, Reading To Learn and Cross-Topic ExerciseDocumento19 páginasSuggested Answers To Exercise, Reading To Learn and Cross-Topic ExerciseBernardAinda não há avaliações
- Cytology CytoskeletonDocumento48 páginasCytology CytoskeletonMitzel Sapalo0% (1)
- Autoimmune Disease MechanismsDocumento6 páginasAutoimmune Disease MechanismsHaliunaa BattulgaAinda não há avaliações
- Plant and Animal Organ Systems and Their Functions (Gas Exchange and Transport/Circulation)Documento24 páginasPlant and Animal Organ Systems and Their Functions (Gas Exchange and Transport/Circulation)Sherry Macalalad GarciaAinda não há avaliações
- Medical Terms PDFDocumento204 páginasMedical Terms PDFrengachen89% (9)
- Pex 09 03Documento4 páginasPex 09 03Illich Ramirez TantaAinda não há avaliações
- Ilovepdf MergedDocumento457 páginasIlovepdf MergedMar LoyolaAinda não há avaliações
- Freiwald 2016 FOAM-RollingDocumento19 páginasFreiwald 2016 FOAM-RollingPedro GouveiaAinda não há avaliações
- Endocrine System Hormones and GlandsDocumento6 páginasEndocrine System Hormones and GlandsFrancine Dominique CollantesAinda não há avaliações
- Plant and Animal Organs Systems P1Documento8 páginasPlant and Animal Organs Systems P1ian laurence pedranoAinda não há avaliações
- Fisiologi Sistem Saraf TepiDocumento19 páginasFisiologi Sistem Saraf TepiNata NayottamaAinda não há avaliações
- Medical Physiology Membrane PotentialsDocumento39 páginasMedical Physiology Membrane PotentialssanggetharAinda não há avaliações
- Prelim HPCTDocumento37 páginasPrelim HPCTMariaangela AliscuanoAinda não há avaliações
- Genetika 1 PDFDocumento13 páginasGenetika 1 PDFTiko ZazadzeAinda não há avaliações
- Self CareDocumento27 páginasSelf CareJessa May RapadasAinda não há avaliações
- Kuliah 2 - CellDocumento57 páginasKuliah 2 - Cellkamalab04Ainda não há avaliações
- Testicular Torsion: Dr. Hari Krismanuel, Sp. B, FinacsDocumento19 páginasTesticular Torsion: Dr. Hari Krismanuel, Sp. B, FinacsVanessa Modi AlverinaAinda não há avaliações
- HematuriaDocumento86 páginasHematuriaMohamad Arif MustaphaAinda não há avaliações
- VahimetsmartinDocumento0 páginaVahimetsmartinAngela PagliusoAinda não há avaliações
- Lesson 10 Brain Parts, Processes and FunctionsDocumento19 páginasLesson 10 Brain Parts, Processes and FunctionsAlfredo ModestoAinda não há avaliações
- The Digestive System LabelDocumento3 páginasThe Digestive System LabelUSMP FN ARCHIVOSAinda não há avaliações
- Bone and muscle structure, function, and developmentDocumento6 páginasBone and muscle structure, function, and developmentLuna ScorpiusAinda não há avaliações
- Assessing the Abdomen: 4 Quadrants and 9 RegionsDocumento54 páginasAssessing the Abdomen: 4 Quadrants and 9 RegionsWilma Acorin OrillinedaAinda não há avaliações
- Study of Animal Type CockroachDocumento34 páginasStudy of Animal Type CockroachDivya ShivkumarAinda não há avaliações
- Medical Terminology For Dummies Cheat SheetDocumento5 páginasMedical Terminology For Dummies Cheat SheetSir SuneAinda não há avaliações
- Activity No. 7.1 BloodDocumento2 páginasActivity No. 7.1 BloodDree SermanAinda não há avaliações
- Chapter 3 Cells and TissuesDocumento2 páginasChapter 3 Cells and TissuesNathaliaAinda não há avaliações
- Digestive System Anatomy and Physiology - NurseslabsDocumento33 páginasDigestive System Anatomy and Physiology - NurseslabsMari FeAinda não há avaliações
- Multiple Choice Questions on Anatomy and PhysiologyDocumento9 páginasMultiple Choice Questions on Anatomy and Physiologyvaibhavi maliAinda não há avaliações