Você também pode gostar
- Manual Máquina Radiofrecuencia Resistiva y CapacitivaDocumento18 páginasManual Máquina Radiofrecuencia Resistiva y CapacitivaInmaAinda não há avaliações
- Lymphedema ReviewDocumento8 páginasLymphedema ReviewSAKAI69Ainda não há avaliações
- Liposuction SurgeryDocumento12 páginasLiposuction SurgerynainacurthberrtAinda não há avaliações
- Lymphedema After Breast Cancer TreatmentDocumento8 páginasLymphedema After Breast Cancer TreatmentGerardo N. Pabón GallinoAinda não há avaliações
- Critical Care of The Vascular Surgery PatientDocumento16 páginasCritical Care of The Vascular Surgery PatientHerbert Baquerizo VargasAinda não há avaliações
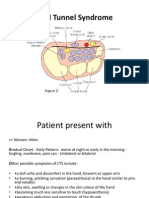
- Carpal Tunnel SyndromeDocumento9 páginasCarpal Tunnel SyndromeselviagandasariAinda não há avaliações
- Physioex Lab Report: Pre-Lab Quiz ResultsDocumento5 páginasPhysioex Lab Report: Pre-Lab Quiz ResultsWilhelm Sánchez100% (1)
- Ift PPT-1Documento21 páginasIft PPT-1Swetha Purushothaman100% (1)
- Micro-Current Natural Facelift Massage: By: Vickie Mickey, CT, CLHRPDocumento17 páginasMicro-Current Natural Facelift Massage: By: Vickie Mickey, CT, CLHRProbertAinda não há avaliações
- Exilis StudieDocumento36 páginasExilis StudiesdwAinda não há avaliações
- Mastery of Vascular and Endovascular SurgeryDocumento751 páginasMastery of Vascular and Endovascular Surgeryadel husseinAinda não há avaliações
- MT9000 UK Manual I-MT9000-UK Rev 2 0213Documento40 páginasMT9000 UK Manual I-MT9000-UK Rev 2 0213Suki YakiAinda não há avaliações
- Weir Et Al. (2019) - Approaching Groin Pain in Athletics 'The Falcon's Perspective'Documento8 páginasWeir Et Al. (2019) - Approaching Groin Pain in Athletics 'The Falcon's Perspective'Tom StevensAinda não há avaliações
- Laser Therapy - SudhaDocumento17 páginasLaser Therapy - SudhaSUDHARSHINI GVAinda não há avaliações
- Chemical Peeling in Ethnic Skin: An Update: What's Already Known About This Topic?Documento9 páginasChemical Peeling in Ethnic Skin: An Update: What's Already Known About This Topic?Rojas Evert AlonsoAinda não há avaliações
- Scoliosis ScreeningDocumento54 páginasScoliosis ScreeningHendra AjahAinda não há avaliações
- LymphedemaDocumento4 páginasLymphedemaSAKAI69Ainda não há avaliações
- Shockwave Therapy MZUEDocumento21 páginasShockwave Therapy MZUELove & HumanityAinda não há avaliações
- Carpal Tunnel Syndrome Power Point PresentationDocumento6 páginasCarpal Tunnel Syndrome Power Point Presentationapi-237061134Ainda não há avaliações
- Interferential Therapy 2021Documento13 páginasInterferential Therapy 2021Mộng HoàngAinda não há avaliações
- Muscle StimulationDocumento15 páginasMuscle StimulationApoorvAinda não há avaliações
- CareTec IV DT4444 ManualDocumento48 páginasCareTec IV DT4444 Manualenergetiko15100% (1)
- Sclerotherapy German GuidelinesDocumento8 páginasSclerotherapy German GuidelinesGabriela DrăgoiAinda não há avaliações
- Gimnasia PasivaDocumento15 páginasGimnasia PasivaCristian AlvarezAinda não há avaliações
- Emily Iker, MD: LymphedemaDocumento37 páginasEmily Iker, MD: LymphedemaJustin HarperAinda não há avaliações
- Surgery IDocumento180 páginasSurgery IFertu CatalinAinda não há avaliações
- Effects of Isometric, Eccentric, or Heavy Slow Resistance Exercises On Pain and Function With PTDocumento15 páginasEffects of Isometric, Eccentric, or Heavy Slow Resistance Exercises On Pain and Function With PTTomBramboAinda não há avaliações
- APA 7th Edition Template Student VersionDocumento14 páginasAPA 7th Edition Template Student VersionAndrei ArtiedaAinda não há avaliações
- By . DR Shivraj Sharma 1 Year Resident Dept - of General Surgery NMCTH, BirgunjDocumento32 páginasBy . DR Shivraj Sharma 1 Year Resident Dept - of General Surgery NMCTH, BirgunjVu ThangAinda não há avaliações
- Bodyter PDFDocumento65 páginasBodyter PDFMihuța NarcisaAinda não há avaliações
- 215 PDFDocumento7 páginas215 PDFlewamAinda não há avaliações
- Compresas Húmedo CalientesDocumento5 páginasCompresas Húmedo CalientesSebastian Ernesto Siegmund SanhuezaAinda não há avaliações
- Lipolytic Laser: Price, Effectiveness and ContraindicationsDocumento1 páginaLipolytic Laser: Price, Effectiveness and ContraindicationsDaniel Fajardo VilacháAinda não há avaliações
- Eng Tecar-Crv-200 Rev1 LRDocumento36 páginasEng Tecar-Crv-200 Rev1 LRThe LamAinda não há avaliações
- Wound Healing: Santos, Patrick John S., MD First Year Resident Department of Surgery Manila MedDocumento60 páginasWound Healing: Santos, Patrick John S., MD First Year Resident Department of Surgery Manila MedJhessie ChingAinda não há avaliações
- A Practical Guide To Kinesiology Taping For Injury Prevention and Common Medical Conditions (John Gibbons) (Z-Library)Documento105 páginasA Practical Guide To Kinesiology Taping For Injury Prevention and Common Medical Conditions (John Gibbons) (Z-Library)alejuan252Ainda não há avaliações
- 2009 4 Laser Lipolysis 1 0Documento13 páginas2009 4 Laser Lipolysis 1 0aillAinda não há avaliações
- General Surgery: Post-Operative Care and ManagementDocumento9 páginasGeneral Surgery: Post-Operative Care and ManagementMohammed Yousif AbdualjabbarAinda não há avaliações
- Liposuccion Alta Definicion PDFDocumento10 páginasLiposuccion Alta Definicion PDFDIOGENESAinda não há avaliações
- Amputation AssignmentDocumento19 páginasAmputation Assignmentmushimiyimana jacquelineAinda não há avaliações
- Manual de Usuario Ipl OptDocumento37 páginasManual de Usuario Ipl OptrudavanegasAinda não há avaliações
- Lymphatic and Vascular System RehabDocumento73 páginasLymphatic and Vascular System RehabWenzy Cruz100% (1)
- Manual Select ComboDocumento44 páginasManual Select ComboGestión Biomédica Norte Salud y CeireAinda não há avaliações
- BURNDocumento35 páginasBURNSri Muliani IdrisAinda não há avaliações
- Return To Play PracticesDocumento12 páginasReturn To Play PracticesAndre LuísAinda não há avaliações
- MOIST HEAT THERAPY & PARAFFIN WAX BATH PresentationDocumento29 páginasMOIST HEAT THERAPY & PARAFFIN WAX BATH PresentationGeddam Snehalatha100% (1)
- Compartment SynDocumento51 páginasCompartment SynFIYINFOLUWA ESTHER AYODELEAinda não há avaliações
- AtaxiaDocumento19 páginasAtaxiaHenry DanielAinda não há avaliações
- Lower Limb ReconstructionDocumento58 páginasLower Limb ReconstructionjibranrabbaniAinda não há avaliações
- Hifu 3DDocumento13 páginasHifu 3DBashir MtwaklAinda não há avaliações
- Whirlpool Bath TherapyDocumento13 páginasWhirlpool Bath TherapyRichaAinda não há avaliações
- Winback - en Brochure Rshock Version J3 Mars 2021 ADocumento12 páginasWinback - en Brochure Rshock Version J3 Mars 2021 AThao Nguyen100% (1)
- Introduction To Physical AgentsDocumento25 páginasIntroduction To Physical AgentsCyril Jay G. OrtegaAinda não há avaliações
- The Relationship Between Heavy Menstrual Bleeding, Iron Deficiency and Iron Deficiency AnemiaDocumento9 páginasThe Relationship Between Heavy Menstrual Bleeding, Iron Deficiency and Iron Deficiency AnemiaKevin Stanley HalimAinda não há avaliações
- Et-Lec 14 Wax TherapyDocumento64 páginasEt-Lec 14 Wax TherapyAngelic khanAinda não há avaliações
- Laser & Light Therapy: Miftahul ZannahDocumento27 páginasLaser & Light Therapy: Miftahul Zannahmiranda salimAinda não há avaliações
- PT Journal Musclel ActivityDocumento8 páginasPT Journal Musclel ActivityKarthigaMurugesanAinda não há avaliações
- Lymph Drainage Therapy PDFDocumento7 páginasLymph Drainage Therapy PDFDiego Mamani Mullisaca100% (2)
- 9-Otros Usos Del UltraSonidoDocumento24 páginas9-Otros Usos Del UltraSonidosantiago jofreAinda não há avaliações
- Class 12 Psychology PDFDocumento209 páginasClass 12 Psychology PDFSoumyashis Bhattacharya0% (1)
- High Voltage Fast-Switching NPN Power Transistor: FeaturesDocumento11 páginasHigh Voltage Fast-Switching NPN Power Transistor: FeaturesVESVOCAinda não há avaliações
- CHAPTER 48 - Skin Integrity & Wound CareDocumento3 páginasCHAPTER 48 - Skin Integrity & Wound CareAAinda não há avaliações
- Morris 2Documento22 páginasMorris 2IsmaelLouGomezAinda não há avaliações
- Astm E1975 - 1 (En)Documento17 páginasAstm E1975 - 1 (En)Dinesh Sai100% (1)
- Lisca - Lingerie Catalog II Autumn Winter 2013Documento76 páginasLisca - Lingerie Catalog II Autumn Winter 2013OvidiuAinda não há avaliações
- Rog Strix Z390-E Gaming: DDR4 4266 Qualified Vendors List (QVL)Documento13 páginasRog Strix Z390-E Gaming: DDR4 4266 Qualified Vendors List (QVL)ALAN ANDRES ZAVALA LLANOSAinda não há avaliações
- Freedom As A Foundation of EthicsDocumento3 páginasFreedom As A Foundation of EthicsGrant Jomar SiadorAinda não há avaliações
- Broadway CafeDocumento13 páginasBroadway CafeIoana Taon100% (1)
- Properties of Equality PDFDocumento1 páginaProperties of Equality PDFR. I. P.Ainda não há avaliações
- MV "RS Mistral": 712 TEU Geared Cellular Container VesselDocumento1 páginaMV "RS Mistral": 712 TEU Geared Cellular Container VesselMeryAinda não há avaliações
- Selulitis Orbita Pada Laki-Laki Usia 64 Tahun: Laporan KasusDocumento8 páginasSelulitis Orbita Pada Laki-Laki Usia 64 Tahun: Laporan KasusLuh Dita YuliandinaAinda não há avaliações
- Bombardier Zefiro Technical Description enDocumento15 páginasBombardier Zefiro Technical Description ennickerlesstezla100% (1)
- HVT DS HAEFELY RIC 422 Reference Impulse Calibrator V2004Documento4 páginasHVT DS HAEFELY RIC 422 Reference Impulse Calibrator V2004leivajAinda não há avaliações
- CPower Product Training.09.2016.EnDocumento70 páginasCPower Product Training.09.2016.Enerdinc100% (1)
- Project Sanjay YadavDocumento51 páginasProject Sanjay YadavriyacomputerAinda não há avaliações
- Essay Flooding and MitigationDocumento3 páginasEssay Flooding and MitigationCindy HosianiAinda não há avaliações
- Colorado Wing - Sep 2012Documento32 páginasColorado Wing - Sep 2012CAP History LibraryAinda não há avaliações
- Seminar 2 of 2021-Multispectral Spectroscopy-Aster Imagery Processing For Mineral ExplorationDocumento15 páginasSeminar 2 of 2021-Multispectral Spectroscopy-Aster Imagery Processing For Mineral Explorationmartin nyakinyeAinda não há avaliações
- Aakash Zoology Study Package 3 SolutionsssssssDocumento104 páginasAakash Zoology Study Package 3 SolutionsssssssRishika PaulAinda não há avaliações
- SG5.0 20RT UEN Ver13 202101Documento105 páginasSG5.0 20RT UEN Ver13 202101Asep SaepudinAinda não há avaliações
- Practice Test 1 + 2Documento19 páginasPractice Test 1 + 2yếnAinda não há avaliações
- A. Questions: Conversation Activities - TravelDocumento11 páginasA. Questions: Conversation Activities - TravelkicsirekaAinda não há avaliações
- OpenSeesPL 5ICEEDocumento6 páginasOpenSeesPL 5ICEEDaniel Hernandez AtencioAinda não há avaliações
- Module I: Introduction To Environmental PollutionDocumento14 páginasModule I: Introduction To Environmental PollutionAman John TuduAinda não há avaliações
- Discussion 2 Module 2 - Paronda PDFDocumento1 páginaDiscussion 2 Module 2 - Paronda PDFAlvanna ParondaAinda não há avaliações
- Operating Manual For Kipor Mobile Gic-Pg Kipor Quick Guide OmDocumento8 páginasOperating Manual For Kipor Mobile Gic-Pg Kipor Quick Guide OmIan CutinAinda não há avaliações
- Constructing 30deg AngleDocumento4 páginasConstructing 30deg AngleArthur ChewAinda não há avaliações
- The Ayurvedic Vegan Kitchen PDFDocumento203 páginasThe Ayurvedic Vegan Kitchen PDFRuvaly MzAinda não há avaliações
- Exam of Refinery PDF 2Documento20 páginasExam of Refinery PDF 2ئارام ناصح محمد حسێن0% (1)