Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 2Documento8 páginasSmall Animal Abdominal Ultrasonography Liver & GallBladder - Part 2ludiegues752100% (1)
- (2015) Basics of Equine DermatologyDocumento10 páginas(2015) Basics of Equine Dermatologyludiegues752Ainda não há avaliações
- Abdominal Ultrasonographic Findings Associated With Feline Infectious Peritonitis PDFDocumento73 páginasAbdominal Ultrasonographic Findings Associated With Feline Infectious Peritonitis PDFludiegues752Ainda não há avaliações
- Powerpoint: Anal and Perianal DisordersDocumento66 páginasPowerpoint: Anal and Perianal Disordersj.doe.hex_8780% (5)
- Diet After Gall Bladder RemovalDocumento5 páginasDiet After Gall Bladder RemovalLaparoscopic surgeon jabalpur digant pathakAinda não há avaliações
- Blumgart PDFDocumento815 páginasBlumgart PDFrensobger87% (15)
- Top 5 Causes of Splenomegaly in Dogs - Clinicians BriefDocumento5 páginasTop 5 Causes of Splenomegaly in Dogs - Clinicians Briefludiegues752Ainda não há avaliações
- Imaging Intestinal ObstructionDocumento5 páginasImaging Intestinal Obstructionludiegues752Ainda não há avaliações
- US Artifacts - University of ChicagoDocumento101 páginasUS Artifacts - University of Chicagoludiegues752Ainda não há avaliações
- Small Animal Abdominal Ultrasonography - The SpleenDocumento9 páginasSmall Animal Abdominal Ultrasonography - The Spleenludiegues752Ainda não há avaliações
- Formulation of A Standardized Protocol and Determination of The Size and Appearance of The Spleen in Healthy CatsDocumento8 páginasFormulation of A Standardized Protocol and Determination of The Size and Appearance of The Spleen in Healthy Catsludiegues752Ainda não há avaliações
- Radiology Packet 7 Congenital Cardiac DiseaseDocumento27 páginasRadiology Packet 7 Congenital Cardiac Diseaseludiegues752Ainda não há avaliações
- Radiology Packet 5 Heart FailureDocumento25 páginasRadiology Packet 5 Heart Failureludiegues752Ainda não há avaliações
- Case Report: Rapport de CasDocumento4 páginasCase Report: Rapport de Casludiegues752Ainda não há avaliações
- (2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in DogsDocumento5 páginas(2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in Dogsludiegues752Ainda não há avaliações
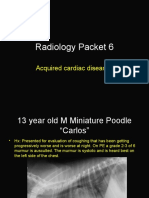
- Radiology Packet 6 Acquired Cardiac DiseasesDocumento25 páginasRadiology Packet 6 Acquired Cardiac Diseasesludiegues752Ainda não há avaliações
- Radiology Packet 4 Cardiac EnlargementDocumento28 páginasRadiology Packet 4 Cardiac Enlargementludiegues752Ainda não há avaliações
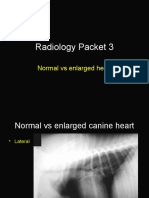
- Radiology Packet 3 Normal Vs Enlarged HeartDocumento11 páginasRadiology Packet 3 Normal Vs Enlarged Heartludiegues752Ainda não há avaliações
- The IntegumentDocumento15 páginasThe Integumentludiegues752Ainda não há avaliações
- Spleen Evaluation Using Contrast Enhanced Ultrasonography and Doppler in Dogs With Subclinical EhrlichiosisDocumento5 páginasSpleen Evaluation Using Contrast Enhanced Ultrasonography and Doppler in Dogs With Subclinical Ehrlichiosisludiegues752Ainda não há avaliações
- Alterations in The SkinDocumento9 páginasAlterations in The Skinludiegues752Ainda não há avaliações
- Derm History FormDocumento1 páginaDerm History Formludiegues752Ainda não há avaliações
- (2016) Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 1Documento7 páginas(2016) Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 1ludiegues752100% (1)
- Nodular Fat Necrosis in The Feline and Canine AbdomenDocumento5 páginasNodular Fat Necrosis in The Feline and Canine Abdomenludiegues752Ainda não há avaliações
- (2015) Part 1 - Basics of Ultrasound Transducers & Image FormationDocumento4 páginas(2015) Part 1 - Basics of Ultrasound Transducers & Image Formationludiegues752Ainda não há avaliações
- Ultrasound of The Thorax (Noncardiac)Documento13 páginasUltrasound of The Thorax (Noncardiac)ludiegues752Ainda não há avaliações
- Ultrasonographic Differences Between Dogs and CatsDocumento13 páginasUltrasonographic Differences Between Dogs and Catsludiegues752Ainda não há avaliações
- Constipation NCPDocumento2 páginasConstipation NCPKaren Pili100% (1)
- What Happens If Anal Fistula Is Not Treated On Time? - Dr. Samrat JankarDocumento3 páginasWhat Happens If Anal Fistula Is Not Treated On Time? - Dr. Samrat JankarDr. Samrat JankarAinda não há avaliações
- LESSON PLAN On PancreasDocumento4 páginasLESSON PLAN On PancreasShweta Pal100% (1)
- Curriculum Dia Rad Gi - Gu RotationDocumento2 páginasCurriculum Dia Rad Gi - Gu Rotationmafsd jlAinda não há avaliações
- Anatomy and PhysiologyDocumento4 páginasAnatomy and PhysiologyJohn Rey Abad67% (3)
- Science 4 4a's CollabDocumento14 páginasScience 4 4a's CollabAr WinAinda não há avaliações
- Short Case - Stoma ExaminationDocumento6 páginasShort Case - Stoma Examination张虢袀Ainda não há avaliações
- Q4 Science 8 Week1Documento4 páginasQ4 Science 8 Week1Mischelle Pumar DyAinda não há avaliações
- Screenshot 2021-10-15 at 23.16.42Documento63 páginasScreenshot 2021-10-15 at 23.16.42Cynthia AristaAinda não há avaliações
- Administration of An Enema: Prepared By: Salwa MaghrabiDocumento16 páginasAdministration of An Enema: Prepared By: Salwa MaghrabiAnonymous 1EoKWlAinda não há avaliações
- CH 26 Student DigestiveDocumento68 páginasCH 26 Student DigestiveMaski03Ainda não há avaliações
- Case Study Fecal EliminationDocumento3 páginasCase Study Fecal EliminationAlyssa Jade GolezAinda não há avaliações
- Gambaran Pola Kehilangan Gigi Sebagian Pada MasyarakatDocumento6 páginasGambaran Pola Kehilangan Gigi Sebagian Pada MasyarakatrahmaAinda não há avaliações
- Indikasi, Teknik Pembuatan Stoma, ReanastomosisDocumento43 páginasIndikasi, Teknik Pembuatan Stoma, ReanastomosiswantoAinda não há avaliações
- Mirizzi Syndrome: A Review of The Literature: January 2006Documento5 páginasMirizzi Syndrome: A Review of The Literature: January 2006Novi WiarniAinda não há avaliações
- Travis Mia Sheridan 4 Ebook Full ChapterDocumento51 páginasTravis Mia Sheridan 4 Ebook Full Chapterdonald.ramirez413100% (5)
- Digestion New BioHackDocumento10 páginasDigestion New BioHackManav SinghAinda não há avaliações
- Abdominal ExaminationDocumento54 páginasAbdominal ExaminationGemmalene Pacleb100% (4)
- Lecture Diarrhea and ConstipationDocumento63 páginasLecture Diarrhea and ConstipationKrittin NaravejsakulAinda não há avaliações
- Chronic DiarrheaDocumento66 páginasChronic DiarrheaJulita Yanti100% (1)
- Classification and Management of Rectal Prolapse After Anorectoplasty For Anorectal MalformationsDocumento8 páginasClassification and Management of Rectal Prolapse After Anorectoplasty For Anorectal MalformationsMarkoAinda não há avaliações
- EHBADocumento14 páginasEHBAJennifer DixonAinda não há avaliações
- Lecture 24, Human-Microbial Interactions - ENDocumento18 páginasLecture 24, Human-Microbial Interactions - ENNariopolusAinda não há avaliações
- Acute Abdominal Bleeding - HandoutDocumento10 páginasAcute Abdominal Bleeding - HandoutMohamed FigoAinda não há avaliações
- Prevalencia de Ulcera Gastrica en Caballos Con Colico EquinoDocumento7 páginasPrevalencia de Ulcera Gastrica en Caballos Con Colico EquinoMaria Paula DuqueAinda não há avaliações
- Esophages and Stomach ...........Documento65 páginasEsophages and Stomach ...........Gebrie DinkayehuAinda não há avaliações
- Cholangiocarcinoma: Presented By: DR Happy Kagathara 4 August, 2012 Dept of GI Surgery Sir Ganga Ram HospitalDocumento96 páginasCholangiocarcinoma: Presented By: DR Happy Kagathara 4 August, 2012 Dept of GI Surgery Sir Ganga Ram HospitalReza SatriaAinda não há avaliações