Você também pode gostar
- Feline Abdominal Ultrasonography: What'S Normal? What'S Abnormal?Documento8 páginasFeline Abdominal Ultrasonography: What'S Normal? What'S Abnormal?Ветеринарная хирургия Dvm Тозлиян И. А.Ainda não há avaliações
- Pancreas: Thomas G. Nyland - John S. MattoonDocumento1 páginaPancreas: Thomas G. Nyland - John S. MattoonpedroAinda não há avaliações
- Porter & Ramirez, 2005 - Equine Neonatal Thoracic and Abdominal UltrasonographyDocumento23 páginasPorter & Ramirez, 2005 - Equine Neonatal Thoracic and Abdominal Ultrasonographyana.d.costaAinda não há avaliações
- Abdominal Radiography in Small Animals: Chris Warren-Smith and Chris LambDocumento8 páginasAbdominal Radiography in Small Animals: Chris Warren-Smith and Chris LambRystha BurgaAinda não há avaliações
- Wale 2016Documento12 páginasWale 2016Radiologi RSPDAinda não há avaliações
- Engineering ApplicationsDocumento19 páginasEngineering ApplicationsChandirasekaran DhakshinamoorthyAinda não há avaliações
- 3 Abdominal Ultrasound Imaging AnatomyDocumento7 páginas3 Abdominal Ultrasound Imaging Anatomyjefaturaimagenologia Hospital NogalarAinda não há avaliações
- Time Imaging .: Ultrasonography Machine For Veterinary ApplicationDocumento22 páginasTime Imaging .: Ultrasonography Machine For Veterinary ApplicationKanhaiyalal RamAinda não há avaliações
- Pleural Ultrasonography: Paul H. Mayo, MD T, Peter Doelken, MDDocumento13 páginasPleural Ultrasonography: Paul H. Mayo, MD T, Peter Doelken, MDmlannesAinda não há avaliações
- UltrasonographyDocumento21 páginasUltrasonographyChecko LatteAinda não há avaliações
- 1999 Bovino Reproducción Ultrasonido PDFDocumento16 páginas1999 Bovino Reproducción Ultrasonido PDFMarco Antonio AspronAinda não há avaliações
- Ultrasonography Principles Indications and Limitations PDFDocumento3 páginasUltrasonography Principles Indications and Limitations PDFMuchtar RezaAinda não há avaliações
- Imaging Modalities of Large Bowel: DR. Srijit SahaDocumento38 páginasImaging Modalities of Large Bowel: DR. Srijit SahasrijitAinda não há avaliações
- Basic Principles of Diagnostic UltrasonographyDocumento5 páginasBasic Principles of Diagnostic UltrasonographyAgung KusastiAinda não há avaliações
- Ultrasonograph yDocumento2 páginasUltrasonograph yAdrin Ma'rufAinda não há avaliações
- Ultrasound Presentation PDFDocumento35 páginasUltrasound Presentation PDFLuqman QadirAinda não há avaliações
- Panduan Pemeriksaan Radiologi Bagi PasienDocumento19 páginasPanduan Pemeriksaan Radiologi Bagi PasienMinto SanjoyoAinda não há avaliações
- Recent Advances in Gynaec UsgDocumento46 páginasRecent Advances in Gynaec UsgKalpavriksha1974Ainda não há avaliações
- Diagnostic Imaging of The Pharynx and Esophagus: Key PointsDocumento33 páginasDiagnostic Imaging of The Pharynx and Esophagus: Key PointsChutcharwan JintasoponAinda não há avaliações
- Abdominal ImagingDocumento45 páginasAbdominal ImagingFahriansyah Mp Tmc100% (1)
- Modifications of X-RayDocumento6 páginasModifications of X-Rayolajumokeojo9Ainda não há avaliações
- Feline AdrenalandsDocumento17 páginasFeline AdrenalandsOlga KucinskaAinda não há avaliações
- Abdomen Protocol CME PDFDocumento6 páginasAbdomen Protocol CME PDFcristinaAinda não há avaliações
- Best Practice & Research Clinical Obstetrics and GynaecologyDocumento19 páginasBest Practice & Research Clinical Obstetrics and GynaecologyJaime Andres Pardo RomeroAinda não há avaliações
- Airway Management Using UltrasoundDocumento7 páginasAirway Management Using Ultrasoundroflova1908Ainda não há avaliações
- In Practice 2012 Scott 12 21Documento9 páginasIn Practice 2012 Scott 12 21ransinghAinda não há avaliações
- Pelvic Floor Ultrasound - A Review - 220211 - 100603Documento24 páginasPelvic Floor Ultrasound - A Review - 220211 - 100603Mariana Larroulet SantanderAinda não há avaliações
- High-Quality Breast Ultrasonography. Radiologic Clinics of North AmericaDocumento8 páginasHigh-Quality Breast Ultrasonography. Radiologic Clinics of North AmericaEduardo Alejandro IIIAinda não há avaliações
- Point-of-Care Ultrasound in The Intensive Care UnitDocumento19 páginasPoint-of-Care Ultrasound in The Intensive Care UnitJose ManuelAinda não há avaliações
- Ultrasonography For The Veterinary Nurse - Frank BuschDocumento2 páginasUltrasonography For The Veterinary Nurse - Frank BuschFrank Busch100% (1)
- Imaging of Urethral Stricture Disease: Conrad Maciejewski, Keith RourkeDocumento8 páginasImaging of Urethral Stricture Disease: Conrad Maciejewski, Keith RourkeGd SuarantaAinda não há avaliações
- Measurement of Ovarian Size and Shape ParametersDocumento7 páginasMeasurement of Ovarian Size and Shape ParametersRamisha RaidaAinda não há avaliações
- Abdominal RadiographDocumento13 páginasAbdominal RadiographBagasAinda não há avaliações
- Current Diagnostic Techniques in Veterinary Surgery PDFDocumento2 páginasCurrent Diagnostic Techniques in Veterinary Surgery PDFKirti JamwalAinda não há avaliações
- Medical Imaging HND 2Documento17 páginasMedical Imaging HND 2titadave2Ainda não há avaliações
- GINECOLOGIEDocumento105 páginasGINECOLOGIEBanaru AnaAinda não há avaliações
- Kevin Santosh Joseph 15M4245Documento12 páginasKevin Santosh Joseph 15M4245Kevin JosephAinda não há avaliações
- Diagnosis of Postoperative Urinary Retention Using A Simplified Ultrasound Bladder Measurement (Anesth Analg 2015)Documento6 páginasDiagnosis of Postoperative Urinary Retention Using A Simplified Ultrasound Bladder Measurement (Anesth Analg 2015)Anonymous hF9HwHVuqAinda não há avaliações
- 1 s2.0 S0016510703025082 MainDocumento8 páginas1 s2.0 S0016510703025082 MainJosé Moreira Lima NetoAinda não há avaliações
- Surgical Pelvic Anatomy in Gynecologic OncologyDocumento7 páginasSurgical Pelvic Anatomy in Gynecologic OncologyLuisa MorenoAinda não há avaliações
- Neonatal and Pediatric Thoracic UltrasonographyDocumento10 páginasNeonatal and Pediatric Thoracic UltrasonographyJHONATAN MATA ARANDAAinda não há avaliações
- Chest - Diaphragmatic Motion Studied by M-Mode Ultrasonography Methods, Reproducibility, and Normal Values PDFDocumento10 páginasChest - Diaphragmatic Motion Studied by M-Mode Ultrasonography Methods, Reproducibility, and Normal Values PDFnirchennAinda não há avaliações
- Sialography CTDocumento4 páginasSialography CTNegin HekmatjooAinda não há avaliações
- Basics of FlourosDocumento35 páginasBasics of FlourosFamousmanAinda não há avaliações
- Transanal Endoscopic MicrosurgeryDocumento27 páginasTransanal Endoscopic MicrosurgerySangita ShahAinda não há avaliações
- Transabdominalultrasoundfor Bowelevaluation: Peter M. Rodgers,, Ratan VermaDocumento16 páginasTransabdominalultrasoundfor Bowelevaluation: Peter M. Rodgers,, Ratan VermaAle SosaAinda não há avaliações
- Atalan 1999Documento5 páginasAtalan 1999Mario NúñezAinda não há avaliações
- Reprod Domestic Animals - 2014 - Ortega Ferrusola - Use of Colour and Spectral Doppler Ultrasonography in StallionDocumento9 páginasReprod Domestic Animals - 2014 - Ortega Ferrusola - Use of Colour and Spectral Doppler Ultrasonography in StallionAmanda CristinaAinda não há avaliações
- Veterinary Diagnostics TechniquesDocumento5 páginasVeterinary Diagnostics Techniquesmarcus ciceroAinda não há avaliações
- Articol ExtensoDocumento5 páginasArticol ExtensoDavid CalinAinda não há avaliações
- Palliative Ultrasound-Guided Endoscopic Diode Laser Ablation of Transitional Cell Carcinomas of The Lower Urinary Tract in Dogs.Documento10 páginasPalliative Ultrasound-Guided Endoscopic Diode Laser Ablation of Transitional Cell Carcinomas of The Lower Urinary Tract in Dogs.Dante Nathaniel FajardoAinda não há avaliações
- Radiography of Abdomen - NDocumento40 páginasRadiography of Abdomen - Nnishandhakal715Ainda não há avaliações
- Radiology of Urinary System I-II - III 2024Documento61 páginasRadiology of Urinary System I-II - III 2024mhmtrgnn67Ainda não há avaliações
- ASA Regional AnesthesiaDocumento10 páginasASA Regional Anesthesiayessy32lAinda não há avaliações
- Imaging and RadiologyDocumento7 páginasImaging and RadiologyOdyAinda não há avaliações
- Jurnal 1 PDFDocumento10 páginasJurnal 1 PDFPutri Dery CahyaniAinda não há avaliações
- Contents - 2016 - Veterinary Clinics of North America Food Animal Practice PDFDocumento4 páginasContents - 2016 - Veterinary Clinics of North America Food Animal Practice PDFfelipeAinda não há avaliações
- White-Paper USAT FinalDocumento11 páginasWhite-Paper USAT FinalmicropocketfilmsAinda não há avaliações
- Diagnostic Operation of The Liver and Techniques of Hepatic ResectionDocumento17 páginasDiagnostic Operation of The Liver and Techniques of Hepatic ResectionjuaoAinda não há avaliações
- Top 5 Causes of Splenomegaly in Dogs - Clinicians BriefDocumento5 páginasTop 5 Causes of Splenomegaly in Dogs - Clinicians Briefludiegues752Ainda não há avaliações
- Imaging Intestinal ObstructionDocumento5 páginasImaging Intestinal Obstructionludiegues752Ainda não há avaliações
- US Artifacts - University of ChicagoDocumento101 páginasUS Artifacts - University of Chicagoludiegues752Ainda não há avaliações
- Small Animal Abdominal Ultrasonography - The SpleenDocumento9 páginasSmall Animal Abdominal Ultrasonography - The Spleenludiegues752Ainda não há avaliações
- Formulation of A Standardized Protocol and Determination of The Size and Appearance of The Spleen in Healthy CatsDocumento8 páginasFormulation of A Standardized Protocol and Determination of The Size and Appearance of The Spleen in Healthy Catsludiegues752Ainda não há avaliações
- Radiology Packet 7 Congenital Cardiac DiseaseDocumento27 páginasRadiology Packet 7 Congenital Cardiac Diseaseludiegues752Ainda não há avaliações
- Radiology Packet 5 Heart FailureDocumento25 páginasRadiology Packet 5 Heart Failureludiegues752Ainda não há avaliações
- Case Report: Rapport de CasDocumento4 páginasCase Report: Rapport de Casludiegues752Ainda não há avaliações
- (2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in DogsDocumento5 páginas(2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in Dogsludiegues752Ainda não há avaliações
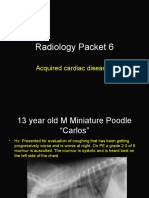
- Radiology Packet 6 Acquired Cardiac DiseasesDocumento25 páginasRadiology Packet 6 Acquired Cardiac Diseasesludiegues752Ainda não há avaliações
- Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 2Documento8 páginasSmall Animal Abdominal Ultrasonography Liver & GallBladder - Part 2ludiegues752100% (1)
- Radiology Packet 4 Cardiac EnlargementDocumento28 páginasRadiology Packet 4 Cardiac Enlargementludiegues752Ainda não há avaliações
- Radiology Packet 3 Normal Vs Enlarged HeartDocumento11 páginasRadiology Packet 3 Normal Vs Enlarged Heartludiegues752Ainda não há avaliações
- (2015) Basics of Equine DermatologyDocumento10 páginas(2015) Basics of Equine Dermatologyludiegues752Ainda não há avaliações
- The IntegumentDocumento15 páginasThe Integumentludiegues752Ainda não há avaliações
- Abdominal Ultrasonographic Findings Associated With Feline Infectious Peritonitis PDFDocumento73 páginasAbdominal Ultrasonographic Findings Associated With Feline Infectious Peritonitis PDFludiegues752Ainda não há avaliações
- Spleen Evaluation Using Contrast Enhanced Ultrasonography and Doppler in Dogs With Subclinical EhrlichiosisDocumento5 páginasSpleen Evaluation Using Contrast Enhanced Ultrasonography and Doppler in Dogs With Subclinical Ehrlichiosisludiegues752Ainda não há avaliações
- Alterations in The SkinDocumento9 páginasAlterations in The Skinludiegues752Ainda não há avaliações
- Derm History FormDocumento1 páginaDerm History Formludiegues752Ainda não há avaliações
- (2016) Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 1Documento7 páginas(2016) Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 1ludiegues752100% (1)
- Nodular Fat Necrosis in The Feline and Canine AbdomenDocumento5 páginasNodular Fat Necrosis in The Feline and Canine Abdomenludiegues752Ainda não há avaliações
- (2015) Part 1 - Basics of Ultrasound Transducers & Image FormationDocumento4 páginas(2015) Part 1 - Basics of Ultrasound Transducers & Image Formationludiegues752Ainda não há avaliações
- Ultrasound of The Thorax (Noncardiac)Documento13 páginasUltrasound of The Thorax (Noncardiac)ludiegues752Ainda não há avaliações
- Ultrasonographic Differences Between Dogs and CatsDocumento13 páginasUltrasonographic Differences Between Dogs and Catsludiegues752Ainda não há avaliações
- Avi Sipermethrin 20 EN MSDSDocumento6 páginasAvi Sipermethrin 20 EN MSDSHasriAAinda não há avaliações
- Daftar Obat DR - Sps DalamDocumento3 páginasDaftar Obat DR - Sps DalamKlinik Sosa Graha MedikaAinda não há avaliações
- Neo Pedia Guidelines Developmental CareDocumento29 páginasNeo Pedia Guidelines Developmental CareUlysses GamayonAinda não há avaliações
- Angiodroid The CO2 Injector - VascupediaDocumento8 páginasAngiodroid The CO2 Injector - VascupediaArnaud TORNIERAinda não há avaliações
- Dilatation and Curettage ProcedureDocumento3 páginasDilatation and Curettage Proceduresagi muAinda não há avaliações
- Drug StudyDocumento3 páginasDrug StudySherlyn Delos ReyesAinda não há avaliações
- Cardiac GlycosidesDocumento5 páginasCardiac Glycosidesapi-347182709100% (1)
- Kuliah Dermato Terapi 2013Documento46 páginasKuliah Dermato Terapi 2013Vania EssiandaAinda não há avaliações
- Teaching Plan For PidDocumento5 páginasTeaching Plan For PidokaciaAinda não há avaliações
- Lifetree Gut Relax, An Ayurvedic Health SupplementDocumento13 páginasLifetree Gut Relax, An Ayurvedic Health SupplementLifetree WorldAinda não há avaliações
- ST 11 Juni-1Documento38 páginasST 11 Juni-1yunannegariAinda não há avaliações
- India's 1 Health Management LabDocumento14 páginasIndia's 1 Health Management LabAjay Kumar dasAinda não há avaliações
- Pham Ngoc Thach University of Medicine DUOC2019Documento109 páginasPham Ngoc Thach University of Medicine DUOC2019Nhung PhamAinda não há avaliações
- Post Term PregnancyDocumento35 páginasPost Term PregnancyNishaThakuri100% (2)
- What Is Anorexia NervosaDocumento2 páginasWhat Is Anorexia NervosaHe DoloresAinda não há avaliações
- Case of Jeannie BrownDocumento1 páginaCase of Jeannie BrownBryan AbestaAinda não há avaliações
- Neurobiology of Hyper ReligiosityDocumento33 páginasNeurobiology of Hyper ReligiosityRavi KumarAinda não há avaliações
- Obstructed Labor & Prolonged LaburDocumento22 páginasObstructed Labor & Prolonged LaburOmari Kabelwa100% (1)
- Working With Whiplash, Part I (Myofascial Techniques)Documento5 páginasWorking With Whiplash, Part I (Myofascial Techniques)Advanced-Trainings.com100% (4)
- Pengaruh Aromaterapi Inhalasi Terhadap Penurunan Nilai Kecemasan Pasien Gagal Ginjal Kronik Yang Menjalani HemodialisaDocumento6 páginasPengaruh Aromaterapi Inhalasi Terhadap Penurunan Nilai Kecemasan Pasien Gagal Ginjal Kronik Yang Menjalani HemodialisaevangelineAinda não há avaliações
- Vitamin C Deficiency: Texts: Text ADocumento21 páginasVitamin C Deficiency: Texts: Text AEduardo Antonio Comaru Gouveia100% (3)
- Delhi Public School, Mathura Road, New Delhi-110003: Health History (Part-I)Documento2 páginasDelhi Public School, Mathura Road, New Delhi-110003: Health History (Part-I)shoaibali09usAinda não há avaliações
- Fluoxetine Duloxetine SertralineDocumento7 páginasFluoxetine Duloxetine SertralineReneé Camille100% (1)
- Radiology ContrastDocumento4 páginasRadiology ContrastsreekaasamAinda não há avaliações
- Factors Influencing Compliance To Dietary Regimen Among Diabetic Patient in Ladoke Akintola University of Technology Teaching Hospital Osogbo. by Folaranmi Basirat TemitopeDocumento98 páginasFactors Influencing Compliance To Dietary Regimen Among Diabetic Patient in Ladoke Akintola University of Technology Teaching Hospital Osogbo. by Folaranmi Basirat TemitopeOMOLOLA ADAMS OLATAYOAinda não há avaliações
- Cognitive Rehab For StrokeDocumento19 páginasCognitive Rehab For StrokeAisyah IcahAinda não há avaliações
- Trauma Radiography Puteri Resort Melaka 2010Documento69 páginasTrauma Radiography Puteri Resort Melaka 2010Syuhada AzmiAinda não há avaliações
- Guidelines On Blood Cultures: Journal of Microbiology, Immunology and InfectionDocumento3 páginasGuidelines On Blood Cultures: Journal of Microbiology, Immunology and InfectionSumesh Shreekhanda ShresthaAinda não há avaliações
- Case Obsos SellyDocumento24 páginasCase Obsos SellyDwi CahyaAinda não há avaliações
- Pediatrics:: History Taking and Physical Examination of AdolescentsDocumento14 páginasPediatrics:: History Taking and Physical Examination of AdolescentsJüdith Marie Reyes BauntoAinda não há avaliações