Você também pode gostar
- WhatsApp Chat With Mrunal KesarkarDocumento4 páginasWhatsApp Chat With Mrunal KesarkarvikasAinda não há avaliações
- Cardiac9RB oilLowersSerumTotalDocumento10 páginasCardiac9RB oilLowersSerumTotalvikasAinda não há avaliações
- xxxxxxxx2827 2019-05-16 872000 PDFDocumento1 páginaxxxxxxxx2827 2019-05-16 872000 PDFvikasAinda não há avaliações
- It CompaniesDocumento7 páginasIt Companiesmack_kk100% (1)
- Pune I PDFDocumento5 páginasPune I PDFvikasAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- GundamDocumento25 páginasGundamBattlecruiser ScharnhorstAinda não há avaliações
- Entropy (Information Theory)Documento17 páginasEntropy (Information Theory)joseph676Ainda não há avaliações
- Al Rafay ProfileDocumento8 páginasAl Rafay ProfileRana UsmanAinda não há avaliações
- Far Eastern University Mba - Thesis 060517Documento2 páginasFar Eastern University Mba - Thesis 060517Lex AcadsAinda não há avaliações
- Musical InstrumentsDocumento23 páginasMusical Instrumentssirius scottAinda não há avaliações
- Australia Harvesting Rainwater For Environment, Conservation & Education: Some Australian Case Studies - University of TechnologyDocumento8 páginasAustralia Harvesting Rainwater For Environment, Conservation & Education: Some Australian Case Studies - University of TechnologyFree Rain Garden ManualsAinda não há avaliações
- Determining Load Ratios For Technical Rescue Systems and EquipmentDocumento2 páginasDetermining Load Ratios For Technical Rescue Systems and EquipmentAhmad Zubair Rasuly0% (1)
- Nemo Outdoor 8.40 User Guide PDFDocumento392 páginasNemo Outdoor 8.40 User Guide PDFXxbugmenotxXAinda não há avaliações
- Ifrs 15Documento24 páginasIfrs 15Madhu Sudan DarjeeAinda não há avaliações
- CIVIL 3811 - Lecture Slides - Week 7Documento58 páginasCIVIL 3811 - Lecture Slides - Week 7hadaAinda não há avaliações
- Glorious Mysteries 1Documento5 páginasGlorious Mysteries 1Vincent safariAinda não há avaliações
- Altium Designer Training For Schematic Capture and PCB EditingDocumento248 páginasAltium Designer Training For Schematic Capture and PCB EditingAntonio Dx80% (5)
- 160 78-m1Documento70 páginas160 78-m1George100% (7)
- Unit 5, Orders and Cover Letters of Orders For StsDocumento13 páginasUnit 5, Orders and Cover Letters of Orders For StsthuhienAinda não há avaliações
- Course: Consumer Behaviour: Relaunching of Mecca Cola in PakistanDocumento10 páginasCourse: Consumer Behaviour: Relaunching of Mecca Cola in PakistanAnasAhmedAinda não há avaliações
- Psych PresurgicalDocumento31 páginasPsych Presurgicalriham ammar100% (1)
- Sullair VARIABLE SPEED - 1800-2200-1800V-1809V-2200V-25-30HPDocumento70 páginasSullair VARIABLE SPEED - 1800-2200-1800V-1809V-2200V-25-30HPJose MontielAinda não há avaliações
- Navigation - Star FinderDocumento31 páginasNavigation - Star FinderPrasadtAinda não há avaliações
- Can J Chem Eng - 2022 - Mocellin - Experimental Methods in Chemical Engineering Hazard and Operability Analysis HAZOPDocumento20 páginasCan J Chem Eng - 2022 - Mocellin - Experimental Methods in Chemical Engineering Hazard and Operability Analysis HAZOPbademmaliAinda não há avaliações
- Hal Foster Vision and Visuality Discussions in Contemporary Culture PDFDocumento75 páginasHal Foster Vision and Visuality Discussions in Contemporary Culture PDFEd GomesAinda não há avaliações
- Shaira Narrative Report (Final)Documento7 páginasShaira Narrative Report (Final)Sheryll TamangAinda não há avaliações
- Application List: Required Items: A: Cpu-95 Ignition ModuleDocumento12 páginasApplication List: Required Items: A: Cpu-95 Ignition ModuleShubra DebAinda não há avaliações
- Data Processing and Management Information System (AvtoBərpaEdilmiş)Documento6 páginasData Processing and Management Information System (AvtoBərpaEdilmiş)2304 Abhishek vermaAinda não há avaliações
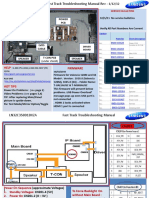
- Samsung LN55C610N1FXZA Fast Track Guide (SM)Documento4 páginasSamsung LN55C610N1FXZA Fast Track Guide (SM)Carlos OdilonAinda não há avaliações
- LP Addition of PolynomialsDocumento5 páginasLP Addition of PolynomialsJolina Bagwisa LptAinda não há avaliações
- Sekonic L 758Documento68 páginasSekonic L 758mariosapereiraAinda não há avaliações
- MGMT 4Documento26 páginasMGMT 4Said GunayAinda não há avaliações
- ns2 LectureDocumento34 páginasns2 LecturedhurgadeviAinda não há avaliações
- Ga2 27:6:23Documento1 páginaGa2 27:6:23john HuntAinda não há avaliações
- MCQ With AnsDocumento8 páginasMCQ With AnsAman KumarAinda não há avaliações