Você também pode gostar
- New Prometric Questions Sample (DHA)Documento7 páginasNew Prometric Questions Sample (DHA)Dr-Usman Khan84% (56)
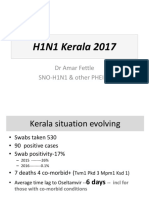
- H1N1 Kerala 2017: DR Amar Fettle SNO-H1N1 & Other PHEICSDocumento21 páginasH1N1 Kerala 2017: DR Amar Fettle SNO-H1N1 & Other PHEICSShamlin OommenAinda não há avaliações
- IELTS Writing Task 2 Workshop PDFDocumento2 páginasIELTS Writing Task 2 Workshop PDFmohammed jebreelAinda não há avaliações
- IELTS Task 1 Writing Band DescriptorsDocumento2 páginasIELTS Task 1 Writing Band Descriptorspelosa12345Ainda não há avaliações
- H1N1 Kerala 2017: DR Amar Fettle SNO-H1N1 & Other PHEICSDocumento21 páginasH1N1 Kerala 2017: DR Amar Fettle SNO-H1N1 & Other PHEICSShamlin OommenAinda não há avaliações
- 1 MCQ Pharmaceutical TechnologyDocumento23 páginas1 MCQ Pharmaceutical TechnologySSB79% (14)
- Pharmacist - Blueprint and Reference (Dec2016) PDFDocumento1 páginaPharmacist - Blueprint and Reference (Dec2016) PDFShamlin OommenAinda não há avaliações
- Pharmacist - Blueprint and Reference (Dec2016)Documento1 páginaPharmacist - Blueprint and Reference (Dec2016)Shamlin OommenAinda não há avaliações
- Fist Ulog RamDocumento5 páginasFist Ulog Ramansmart997373Ainda não há avaliações
- Cover LetterDocumento1 páginaCover LetterShamlin OommenAinda não há avaliações
- Cover LetterDocumento1 páginaCover LetterShamlin OommenAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Drug Study 8Documento3 páginasDrug Study 8Vicky RoqueAinda não há avaliações
- Chapter7 B and T Cell Activation (1) ImmunologyDocumento21 páginasChapter7 B and T Cell Activation (1) ImmunologyIka BakarAinda não há avaliações
- Prevention of Ebola Virus InfectionDocumento55 páginasPrevention of Ebola Virus InfectionAnusha VergheseAinda não há avaliações
- Asthma2 Case StudyDocumento8 páginasAsthma2 Case StudyGlenn Asuncion PagaduanAinda não há avaliações
- ID Consult TemplateDocumento5 páginasID Consult TemplateRohitKumar100% (1)
- Module Description. Pathology of Musculosceletal SystemDocumento52 páginasModule Description. Pathology of Musculosceletal SystemAlberto MayorgaAinda não há avaliações
- Askep CKDDocumento55 páginasAskep CKDyuli ariyantiAinda não há avaliações
- PG - 2016 - 2017 SESSION List of Candidates Allotted - On 11.04.2016Documento16 páginasPG - 2016 - 2017 SESSION List of Candidates Allotted - On 11.04.2016chenda raviAinda não há avaliações
- Acu-Stim For RecoveryDocumento4 páginasAcu-Stim For Recoverycare_e_genAinda não há avaliações
- Shwayder, T., Schneider, S. L., Icecreamwala, D., & Jahnke, M. N. (2019) - Longitudinal Observation of Pediatric Dermatology Patients.Documento255 páginasShwayder, T., Schneider, S. L., Icecreamwala, D., & Jahnke, M. N. (2019) - Longitudinal Observation of Pediatric Dermatology Patients.Cristina GilcaAinda não há avaliações
- Methods of Nutrient DeliveryDocumento3 páginasMethods of Nutrient DeliveryFarmisa MannanAinda não há avaliações
- Common Poison in ChildrenDocumento31 páginasCommon Poison in ChildrenNimi BatuboAinda não há avaliações
- Precosious Puberty Case StudyDocumento27 páginasPrecosious Puberty Case Studynishavohreh100% (1)
- ISR NG Chun Ruh2Documento1 páginaISR NG Chun Ruh2Yasmine SlhAinda não há avaliações
- Step by Step Root Canal TreatmentDocumento157 páginasStep by Step Root Canal TreatmentKaaroma Tamoaieta100% (1)
- Acute Stress Disorder 1Documento22 páginasAcute Stress Disorder 1Seiska MegaAinda não há avaliações
- LAB 4 Simple Stain 2nd 2020-2021Documento17 páginasLAB 4 Simple Stain 2nd 2020-2021Deena Hajj QasemAinda não há avaliações
- Perspective: New England Journal MedicineDocumento4 páginasPerspective: New England Journal MedicineGary MaoAinda não há avaliações
- 5 Weight LossDocumento41 páginas5 Weight LossTasniiem KhmbataAinda não há avaliações
- Sarhad 8MCF BadlmaDocumento29 páginasSarhad 8MCF Badlmasoran najebAinda não há avaliações
- 11 Grammar Test: 94 Photocopiable © Oxford University PressDocumento1 página11 Grammar Test: 94 Photocopiable © Oxford University PressLauri RosseAinda não há avaliações
- Bacterial Skin and Soft Tissue Infections: Clinical Review ArticleDocumento9 páginasBacterial Skin and Soft Tissue Infections: Clinical Review ArticleRini MayaSariAinda não há avaliações
- I Nengah Kundera, Mursito Bialangi: 1. PendahuluanDocumento6 páginasI Nengah Kundera, Mursito Bialangi: 1. PendahuluanDesak Putu Widya AprilianiAinda não há avaliações
- How Can Help You?: A You A You A You A YouDocumento1 páginaHow Can Help You?: A You A You A You A Youimpresiv MAinda não há avaliações
- Activity Intolerance YAp ER NCPDocumento2 páginasActivity Intolerance YAp ER NCPmecz26100% (2)
- Care Plan TemplateDocumento8 páginasCare Plan TemplateXosweetbebeAinda não há avaliações
- Personal Notes Excpetional StuffDocumento352 páginasPersonal Notes Excpetional StuffYagyeshAinda não há avaliações
- Exosome-Based Immunotherapy: A Promising Approach For Cancer TreatmentDocumento16 páginasExosome-Based Immunotherapy: A Promising Approach For Cancer Treatment1810 15Marvin LionelAinda não há avaliações
- Role of MDCT in Coronary Artery Disease: Swachchhanda Songmen 2071Documento63 páginasRole of MDCT in Coronary Artery Disease: Swachchhanda Songmen 2071Dr KhanAinda não há avaliações
- For Demo in Teaching Strategies by Mike ReyesDocumento10 páginasFor Demo in Teaching Strategies by Mike ReyesPaulo Sandino GaliciaAinda não há avaliações