Você também pode gostar
- 2017 Commercial & Industrial Common Interest Development ActNo Everand2017 Commercial & Industrial Common Interest Development ActAinda não há avaliações
- ESIC Conribution Transfer Letter PDFDocumento2 páginasESIC Conribution Transfer Letter PDFPrashant BedaseAinda não há avaliações
- Sample Filled ESIC Contribution Transfer FormDocumento2 páginasSample Filled ESIC Contribution Transfer FormNagaraju EsikeAinda não há avaliações
- 138 NoticeDocumento3 páginas138 Noticeaman sheikhAinda não há avaliações
- Form of Pension Proposals FormDocumento14 páginasForm of Pension Proposals Formlakshmi naryanaAinda não há avaliações
- Impacts of Claim Settlements On Profitability in The Nigerian Insurance IndustryDocumento63 páginasImpacts of Claim Settlements On Profitability in The Nigerian Insurance IndustrySinmiloluwa S.Ainda não há avaliações
- Form F PDFDocumento2 páginasForm F PDFSatish Sati100% (1)
- Gratuity Form FDocumento2 páginasGratuity Form Fचेतांश सिंह कुशवाह100% (1)
- E-Nomination Facility by Epfo On Unified Member PortalDocumento10 páginasE-Nomination Facility by Epfo On Unified Member PortalUpasana Talapady100% (2)
- Almost Everything You Wanted To Know About PTODocumento34 páginasAlmost Everything You Wanted To Know About PTOpemmaiahAinda não há avaliações
- Esic ChallanDocumento7 páginasEsic Challanrgsr2008Ainda não há avaliações
- Employees' State Insurance Corporation E-Pehchan CardDocumento3 páginasEmployees' State Insurance Corporation E-Pehchan CardAadil HashmiAinda não há avaliações
- Employee Provident FundDocumento7 páginasEmployee Provident FundAkm Ashraf Uddin0% (1)
- Kar Shops Commercial Forms FormatDocumento16 páginasKar Shops Commercial Forms FormatbelvaisudheerAinda não há avaliações
- Company Credit Account ApprobationDocumento1 páginaCompany Credit Account ApprobationkiranrauniyarAinda não há avaliações
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocumento3 páginasEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationGoutam HotaAinda não há avaliações
- USSP User Manual v1.0Documento18 páginasUSSP User Manual v1.0Siva ChAinda não há avaliações
- Online Registration of Establishment With DSC: User ManualDocumento39 páginasOnline Registration of Establishment With DSC: User ManualroseAinda não há avaliações
- E Nomination PDFDocumento2 páginasE Nomination PDFSagar RajputAinda não há avaliações
- PF Pension Settlement Form-TCSDocumento4 páginasPF Pension Settlement Form-TCSSridhara Krishna BodavulaAinda não há avaliações
- Form 13Documento3 páginasForm 13ArunAinda não há avaliações
- Taxability of Provident FundDocumento3 páginasTaxability of Provident FundRupen ChawlaAinda não há avaliações
- Insurance BasicsDocumento228 páginasInsurance BasicsLalit SharmaAinda não há avaliações
- Statutory ComplianceDocumento2 páginasStatutory Compliancemax997Ainda não há avaliações
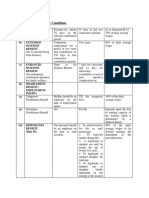
- Benefits & Contributory Conditions: (I) (A) Sickness BenefitDocumento4 páginasBenefits & Contributory Conditions: (I) (A) Sickness BenefitKunwar Sa Amit SinghAinda não há avaliações
- Income Under The Head "Salaries": Shubhangi Gupta Roll No. 11 Financial Management Bhartiya Vidya BhavanDocumento44 páginasIncome Under The Head "Salaries": Shubhangi Gupta Roll No. 11 Financial Management Bhartiya Vidya Bhavanhny0910Ainda não há avaliações
- M.c.theory Claim LetterDocumento11 páginasM.c.theory Claim LetterSandeep DabhiAinda não há avaliações
- Guidelines For The Implementation of A Drug-Free Workplace Policies and Programs For The Private SectorDocumento4 páginasGuidelines For The Implementation of A Drug-Free Workplace Policies and Programs For The Private SectorGerard Nelson ManaloAinda não há avaliações
- Employers Provident Fund (Epf) : Employer CoverageDocumento8 páginasEmployers Provident Fund (Epf) : Employer Coveragevarunreddycool0% (1)
- Payment Payment: Colorado Individual Income Tax Filing GuideDocumento40 páginasPayment Payment: Colorado Individual Income Tax Filing Guidestop recordsAinda não há avaliações
- Gratuity-Form Form FDocumento3 páginasGratuity-Form Form FData. GetAinda não há avaliações
- GGDocumento7 páginasGGVincent CastilloAinda não há avaliações
- Artifact 5 - Employee Pension Scheme Form 10 CDocumento4 páginasArtifact 5 - Employee Pension Scheme Form 10 CSiva chowdaryAinda não há avaliações
- Guidelines and Joining Kit For New JoineesDocumento3 páginasGuidelines and Joining Kit For New JoineesGaurav KumarAinda não há avaliações
- RegistrationDocumento15 páginasRegistrationpratikdhond100% (3)
- Research of Epfo ApprovalDocumento1 páginaResearch of Epfo ApprovalKbg GangadharAinda não há avaliações
- Sallary AllowanceDocumento15 páginasSallary AllowanceKeval PatelAinda não há avaliações
- Workers' CompensationDocumento17 páginasWorkers' CompensationAnele CatayasAinda não há avaliações
- What Is A Flexible Benefit Plan in A Salary Breakup? - QuoraDocumento8 páginasWhat Is A Flexible Benefit Plan in A Salary Breakup? - QuoraSiAinda não há avaliações
- What Types of Benefits Does California Workers' Compensation Pay?Documento5 páginasWhat Types of Benefits Does California Workers' Compensation Pay?Mona DeldarAinda não há avaliações
- Maruti Insurance Broking PVT LTD - MISP - OrDER 227 DTD 17-12-2019Documento13 páginasMaruti Insurance Broking PVT LTD - MISP - OrDER 227 DTD 17-12-2019Moneylife FoundationAinda não há avaliações
- Latest Updates Developments On IRDAIDocumento23 páginasLatest Updates Developments On IRDAINarashimhalu RameshAinda não há avaliações
- Unit 4 Deductions From Gross Total IncomeDocumento31 páginasUnit 4 Deductions From Gross Total IncomeDisha GuptaAinda não há avaliações
- Higher Pension As Per SC Decision With Calculation - Synopsis1Documento13 páginasHigher Pension As Per SC Decision With Calculation - Synopsis1hariveerAinda não há avaliações
- Payroll Taxes in U.SDocumento6 páginasPayroll Taxes in U.SLokesh ChittoraAinda não há avaliações
- ESI Form 5Documento4 páginasESI Form 5savita17julyAinda não há avaliações
- Income Tax and PF, ESIC Due DatesDocumento40 páginasIncome Tax and PF, ESIC Due DatesEXELIENT TAX SERVICESAinda não há avaliações
- CTS Marriage Loan PolicyDocumento5 páginasCTS Marriage Loan PolicyshaannivasAinda não há avaliações
- Register A Transport Company in KenyaDocumento16 páginasRegister A Transport Company in KenyaSamsonAinda não há avaliações
- Income Tax DepartmentDocumento19 páginasIncome Tax DepartmentSharathAinda não há avaliações
- Karnataka Shops and Commercial Establishments Act, 1961Documento44 páginasKarnataka Shops and Commercial Establishments Act, 1961Latest Laws TeamAinda não há avaliações
- Payment of Bonus Act 1965Documento39 páginasPayment of Bonus Act 1965Manojkumar MohanasundramAinda não há avaliações
- PF Nomination FormDocumento3 páginasPF Nomination FormNarendra GaurAinda não há avaliações
- Wipro in PF Settle FormDocumento2 páginasWipro in PF Settle Formumesh100% (1)
- All FormsDocumento27 páginasAll FormsSathyanarayana Reddy Antham100% (1)
- Template - EPFS Form 13 (Revised)Documento3 páginasTemplate - EPFS Form 13 (Revised)Sugam KhetrapalAinda não há avaliações
- 3 - ForM F Gratuity (Sample)Documento4 páginas3 - ForM F Gratuity (Sample)Rajdeep GaharwarAinda não há avaliações
- Employee Self Verification FormDocumento6 páginasEmployee Self Verification Formdharsan321Ainda não há avaliações
- ESIC Conribution Transfer Letter PDFDocumento2 páginasESIC Conribution Transfer Letter PDFPrashant Bedase100% (2)
- Death Claim Form Under Special Cases (Natural Disaster, Calamities, Bomb Blast) - With 1Documento2 páginasDeath Claim Form Under Special Cases (Natural Disaster, Calamities, Bomb Blast) - With 1raviAinda não há avaliações
- Evolution of FJGADDDocumento1 páginaEvolution of FJGADDStewart Paul Tolosa TorreAinda não há avaliações
- Model Constitution of A Community Based Organisation As Water Services ProviderDocumento13 páginasModel Constitution of A Community Based Organisation As Water Services ProviderSanango DavidAinda não há avaliações
- Magendran Mohan V PPDocumento23 páginasMagendran Mohan V PPSyaheera RosliAinda não há avaliações
- Implementation of StrategicDocumento5 páginasImplementation of StrategicAnjang PranataAinda não há avaliações
- In Re Javier-IbayDocumento4 páginasIn Re Javier-Ibaychrisv888Ainda não há avaliações
- Skidgel v. Maine HHS & Ives, 1st Cir. (1993)Documento46 páginasSkidgel v. Maine HHS & Ives, 1st Cir. (1993)Scribd Government DocsAinda não há avaliações
- Conditional Deed of Sale-FinalDocumento3 páginasConditional Deed of Sale-FinalHarold EstacioAinda não há avaliações
- SpColumn ManualDocumento111 páginasSpColumn Manualeid ibrahimAinda não há avaliações
- AUB Tuition Calculator: Provide Some Extra Info For Cost CalculationDocumento1 páginaAUB Tuition Calculator: Provide Some Extra Info For Cost Calculationrony chidiacAinda não há avaliações
- United States v. Demetrius Spence, 4th Cir. (2014)Documento12 páginasUnited States v. Demetrius Spence, 4th Cir. (2014)Scribd Government DocsAinda não há avaliações
- Zzsample - Affidavit of JoinderDocumento4 páginasZzsample - Affidavit of Joinderapi-3744408100% (2)
- RioferioDocumento7 páginasRioferioSocAinda não há avaliações
- 7.3 Caught and Then - Text and QuestionsDocumento6 páginas7.3 Caught and Then - Text and QuestionsToonen BoileyAinda não há avaliações
- Bachelor of Laws Curriculum PDFDocumento3 páginasBachelor of Laws Curriculum PDFAsenath GuiaAinda não há avaliações
- J 1468-2230 1968 tb01206 XDocumento31 páginasJ 1468-2230 1968 tb01206 XMacDonaldAinda não há avaliações
- EJ - 130 Writ of ExecutionDocumento2 páginasEJ - 130 Writ of ExecutionKevin TalbertAinda não há avaliações
- Legal CounselingDocumento106 páginasLegal CounselingCarloErica Austria TambioAdapAinda não há avaliações
- Utilidad Neta RENDIMIENTO FINANCIERO - X 100 VentasDocumento1 páginaUtilidad Neta RENDIMIENTO FINANCIERO - X 100 VentasWilliam AbarcaAinda não há avaliações
- Bengzon vs. Drilon, 208 SCRA 133, April 15, 1992Documento14 páginasBengzon vs. Drilon, 208 SCRA 133, April 15, 1992Edgar Joshua TimbangAinda não há avaliações
- JVD 5 Step Verification ApplicationDocumento2 páginasJVD 5 Step Verification ApplicationRaj Tej75% (4)
- DT Concept BookDocumento268 páginasDT Concept BookAk KhanAinda não há avaliações
- KP FORM #2 AppointmentDocumento10 páginasKP FORM #2 Appointmentahimuro23Ainda não há avaliações
- US Internal Revenue Service: f4868Documento4 páginasUS Internal Revenue Service: f4868IRSAinda não há avaliações
- (U) Daily Activity Report: Marshall DistrictDocumento5 páginas(U) Daily Activity Report: Marshall DistrictFauquier NowAinda não há avaliações
- Campbell V MGN LTD (2004) UKHL 22Documento23 páginasCampbell V MGN LTD (2004) UKHL 22Chaddy123Ainda não há avaliações
- AAR Simultaneous Fire Drill 2019Documento4 páginasAAR Simultaneous Fire Drill 2019Macabebe Fire StationAinda não há avaliações
- CSC Leave FormSDocumento4 páginasCSC Leave FormSHazel NatanauanAinda não há avaliações
- Article 502. The Following Are of PublicDocumento3 páginasArticle 502. The Following Are of PublicrheaAinda não há avaliações
- Justice Dept. Appeal of NY Iphone RulingDocumento150 páginasJustice Dept. Appeal of NY Iphone RulingCNET NewsAinda não há avaliações
- Dar Ao2 02-2009Documento148 páginasDar Ao2 02-2009Angela CanaresAinda não há avaliações