Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The ABC of CBC Interpretation of PDFDocumento193 páginasThe ABC of CBC Interpretation of PDFcarreiromanuel100% (3)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Asociacion de Anticoagulacion-Ppi y Hospitalización Por HdsDocumento12 páginasAsociacion de Anticoagulacion-Ppi y Hospitalización Por HdscarreiromanuelAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Lesiones Esofagicas Manejo ProtesisDocumento5 páginasLesiones Esofagicas Manejo ProtesiscarreiromanuelAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Asociacion de Anticoagulacion-Ppi y Hospitalización Por HDS PDFDocumento10 páginasAsociacion de Anticoagulacion-Ppi y Hospitalización Por HDS PDFcarreiromanuelAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Hemorragia Digestiva Variceal Importancia Momento EndosDocumento16 páginasHemorragia Digestiva Variceal Importancia Momento EndoscarreiromanuelAinda não há avaliações
- Non Alcoholic Fatty Liver DiseaseDocumento16 páginasNon Alcoholic Fatty Liver DiseasecarreiromanuelAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Hemorragia Digestiva Variceal Importancia Momento Endos PDFDocumento10 páginasHemorragia Digestiva Variceal Importancia Momento Endos PDFcarreiromanuelAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Obstetrics en PDFDocumento271 páginasObstetrics en PDFjuitaAinda não há avaliações
- AchalasiaDocumento12 páginasAchalasiacarreiromanuelAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Acido Urico Terapias para Bajar ElDocumento8 páginasAcido Urico Terapias para Bajar ElcarreiromanuelAinda não há avaliações
- Navy Supplement To The DOD Dictionary of Military and Associated Terms, 2011Documento405 páginasNavy Supplement To The DOD Dictionary of Military and Associated Terms, 2011bateljupko100% (1)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- In-Service Welding of Pipelines Industry Action PlanDocumento13 páginasIn-Service Welding of Pipelines Industry Action Planعزت عبد المنعم100% (1)
- SR6 Core Rulebook Errata Feb 2020Documento6 páginasSR6 Core Rulebook Errata Feb 2020yrtalienAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
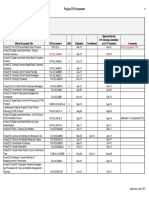
- Project Title Discipline Project Stage Client Attendance CirculationDocumento4 páginasProject Title Discipline Project Stage Client Attendance CirculationgregAinda não há avaliações
- Iron Ore ProcessDocumento52 páginasIron Ore Processjafary448067% (3)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- QuantAssay Software Manual 11-Mar-2019Documento51 páginasQuantAssay Software Manual 11-Mar-2019LykasAinda não há avaliações
- Sci NB Mod 2 LSN 3Documento4 páginasSci NB Mod 2 LSN 3Ramses octavio Rodriguez ocanasAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hurricanes Grade5Documento3 páginasHurricanes Grade5Anonymous m3yrUPAinda não há avaliações
- Communication Models in Internet of Things: A SurveyDocumento5 páginasCommunication Models in Internet of Things: A SurveyIJSTEAinda não há avaliações
- Sch3u Exam Review Ws s2018 PDFDocumento4 páginasSch3u Exam Review Ws s2018 PDFwdsfAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Generative Shape DesignDocumento195 páginasGenerative Shape DesignAdi Fiera100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Procter and Gamble-1Documento5 páginasProcter and Gamble-1Abegiel MendozaAinda não há avaliações
- Nicholas Hudson - From Nation To Race: The Origin of Racial Classification in Eighteenth-CenturyDocumento19 páginasNicholas Hudson - From Nation To Race: The Origin of Racial Classification in Eighteenth-CenturyPedro IIAinda não há avaliações
- John Sisler CISSP Study GuideDocumento126 páginasJohn Sisler CISSP Study GuideAnthonyAinda não há avaliações
- L2 Biostatistics ProbabilityDocumento84 páginasL2 Biostatistics ProbabilityAaron CiudadAinda não há avaliações
- Math 202 Syllabus-Spring18 PDFDocumento2 páginasMath 202 Syllabus-Spring18 PDFvonacoc49Ainda não há avaliações
- ChipmunkDocumento19 páginasChipmunkema.nemec13Ainda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Unit 2 - Presentations (Image, Impact and Making An Impression) 2Documento25 páginasUnit 2 - Presentations (Image, Impact and Making An Impression) 2LK Chiarra Panaligan100% (1)
- History and Philo of ScienceDocumento5 páginasHistory and Philo of ScienceJan Oliver YaresAinda não há avaliações
- CAC Bubble DiagramsDocumento12 páginasCAC Bubble Diagramsangst6250Ainda não há avaliações
- Understanding Bernoulli's Principle Through Simulations PDFDocumento4 páginasUnderstanding Bernoulli's Principle Through Simulations PDFIoannis GaroufalidisAinda não há avaliações
- History of Flash Part - 2Documento7 páginasHistory of Flash Part - 2YOGESHWER NATH SINGHAinda não há avaliações
- CE Review GEOMETRY 2Documento6 páginasCE Review GEOMETRY 2Paul Gerard AguilarAinda não há avaliações
- Approved Project 25 StandardsDocumento5 páginasApproved Project 25 StandardsepidavriosAinda não há avaliações
- DEEP ECOLOGY - An Intro - McLaughlinDocumento5 páginasDEEP ECOLOGY - An Intro - McLaughlinCarlo MagcamitAinda não há avaliações
- Mpfic54 PDFDocumento201 páginasMpfic54 PDFAmy100% (1)
- Tran-Effects of Assisted JumpingDocumento5 páginasTran-Effects of Assisted JumpingyoungjessAinda não há avaliações
- Multiple Choice Enzymes Plant and Animal NutritionDocumento44 páginasMultiple Choice Enzymes Plant and Animal Nutritionliufanjing07Ainda não há avaliações
- Sw34 Religion, Secularism and The Environment by NasrDocumento19 páginasSw34 Religion, Secularism and The Environment by Nasrbawah61455Ainda não há avaliações