Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Anterior Cervical Wall Rupture As A Result of Induced AbortionDocumento4 páginasAnterior Cervical Wall Rupture As A Result of Induced AbortionnawriirwanAinda não há avaliações
- Defisiensi VitaminDocumento30 páginasDefisiensi VitaminnawriirwanAinda não há avaliações
- Fever Sepsis SyokDocumento40 páginasFever Sepsis SyoknawriirwanAinda não há avaliações
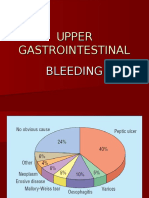
- Upper Gi BleedingDocumento35 páginasUpper Gi Bleedingnawriirwan100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Brochure - Citadines Flatiron Phnom Penh - EnglishDocumento4 páginasBrochure - Citadines Flatiron Phnom Penh - EnglishTix VirakAinda não há avaliações
- 2017 Hyundai Sonata L4-2.4L Engine Controls (Powertrain Management) - ALLDATA RepairDocumento6 páginas2017 Hyundai Sonata L4-2.4L Engine Controls (Powertrain Management) - ALLDATA RepairChino PlagaAinda não há avaliações
- Vet CareplanexampleDocumento6 páginasVet CareplanexampleAnonymous eJZ5HcAinda não há avaliações
- PerthDocumento21 páginasPerthjohn_wlmns3929Ainda não há avaliações
- Heil 4000 FeaturesDocumento1 páginaHeil 4000 FeaturesBogdan NgrAinda não há avaliações
- Line CodingDocumento27 páginasLine CodingshridonAinda não há avaliações
- Jurnal Semi FowlerDocumento6 páginasJurnal Semi FowlerHartina RolobessyAinda não há avaliações
- Soul Wars - Wrath of EverchosenDocumento107 páginasSoul Wars - Wrath of EverchosenRyan BelandAinda não há avaliações
- SpiralsDocumento12 páginasSpiralskkglobalAinda não há avaliações
- A Bilateral Subdural Hematoma Case Report 2165 7548.1000112 PDFDocumento2 páginasA Bilateral Subdural Hematoma Case Report 2165 7548.1000112 PDFPutra GagahAinda não há avaliações
- TNB Ar2011Documento334 páginasTNB Ar2011Duncan LeeAinda não há avaliações
- Unit-4 - Hypothesis TestingDocumento24 páginasUnit-4 - Hypothesis TestingMANTHAN JADHAVAinda não há avaliações
- Zelio Control Relays - RM22TR33Documento7 páginasZelio Control Relays - RM22TR33SIVARAMANJAGANATHANAinda não há avaliações
- Mice and Men Naturalism Web SiteDocumento10 páginasMice and Men Naturalism Web SitedrooolAinda não há avaliações
- ABB Photovoltaic DisconnectorsDocumento6 páginasABB Photovoltaic DisconnectorsBog PenAinda não há avaliações
- Run Omega Run Lunar Omegaverse Book 5 Shyla Colt All ChapterDocumento52 páginasRun Omega Run Lunar Omegaverse Book 5 Shyla Colt All Chapterkate.brown975100% (6)
- Chapter Eight - Vapour Compression CycleDocumento37 páginasChapter Eight - Vapour Compression Cyclealhusseny100% (1)
- GPT Protocol - Trypcase Soy AgarDocumento8 páginasGPT Protocol - Trypcase Soy AgarmailboxofmurliAinda não há avaliações
- The Physiology of Potassium in Crop Production PDFDocumento31 páginasThe Physiology of Potassium in Crop Production PDFFelipe R. Parada100% (1)
- Ycaj CHILLERDocumento108 páginasYcaj CHILLERAbhilash Joseph100% (2)
- Origami PapiroflexiaDocumento6 páginasOrigami PapiroflexiaBraulio RomeroAinda não há avaliações
- Hypochondriasis and Health Anxiety - A Guide For Clinicians (PDFDrive)Documento289 páginasHypochondriasis and Health Anxiety - A Guide For Clinicians (PDFDrive)Fernanda SilvaAinda não há avaliações
- Manuel D'utilisation Maison AnglaisDocumento17 páginasManuel D'utilisation Maison AnglaisVanesssAinda não há avaliações
- Pakistan PresentationDocumento17 páginasPakistan PresentationYaseen Khan100% (1)
- 3 Particle Nature of Matter PDFDocumento4 páginas3 Particle Nature of Matter PDFAtheer AlaniAinda não há avaliações
- DE (Diatomaceous Earth) BenefitsDocumento9 páginasDE (Diatomaceous Earth) BenefitsIlqa116100% (1)
- 7UM512 CatalogueDocumento12 páginas7UM512 Cataloguebuianhtuan1980Ainda não há avaliações
- 03N - Top Level View of Computer Function and InterconnectionDocumento38 páginas03N - Top Level View of Computer Function and InterconnectionDoc TelAinda não há avaliações
- Paracetamol BPDocumento4 páginasParacetamol BPjaimurugeshAinda não há avaliações
- 120Documento349 páginas120xdyj2005Ainda não há avaliações