Você também pode gostar
- Mark Klimek Yellow BookDocumento5 páginasMark Klimek Yellow Bookmaniz44295% (19)
- Sports Injuries - Mechanisms, Prevention and Treatment 2nd Ed - F. Fu, D. Stone Lippincott 1994) WWDocumento1.025 páginasSports Injuries - Mechanisms, Prevention and Treatment 2nd Ed - F. Fu, D. Stone Lippincott 1994) WWplatonRO100% (1)
- Small Animal Anesthesia and Pain Management, Second Edition PDFDocumento473 páginasSmall Animal Anesthesia and Pain Management, Second Edition PDFJorge MázereAinda não há avaliações
- Heart Failure Topic DiscussionDocumento11 páginasHeart Failure Topic Discussionapi-665372449Ainda não há avaliações
- Diabetes Topic DiscussionDocumento9 páginasDiabetes Topic DiscussionSamAinda não há avaliações
- 2 0CommDiseaseIMPTVisionDocumento3 páginas2 0CommDiseaseIMPTVisionAndrea Patricia DaquialAinda não há avaliações
- Soal MAYO Yg KeluarDocumento8 páginasSoal MAYO Yg KeluardoktersaktiAinda não há avaliações
- Implant Manual Reply200DRDocumento50 páginasImplant Manual Reply200DRSrajner Péter100% (1)
- 1183 - The Global Burden of Heart Failure. - Martin COWIE (London, United Kingdom)Documento21 páginas1183 - The Global Burden of Heart Failure. - Martin COWIE (London, United Kingdom)Mulyani EdwarAinda não há avaliações
- Kathrine O Neal PP PDFDocumento92 páginasKathrine O Neal PP PDFrezqAinda não há avaliações
- CPG - Pneumonia (2010 Update)Documento55 páginasCPG - Pneumonia (2010 Update)Jade Kenneth Gonzales LomansocAinda não há avaliações
- Dapa CKDDocumento11 páginasDapa CKDCarlos Andres Tejeda PerezAinda não há avaliações
- IV PO Conversion CAPDocumento3 páginasIV PO Conversion CAPdamondouglasAinda não há avaliações
- SGLT 2 Inhibitors: Newer Paradigms in The Treatment of Heart Failure With Reduced Ejection FractionDocumento4 páginasSGLT 2 Inhibitors: Newer Paradigms in The Treatment of Heart Failure With Reduced Ejection FractionIJAR JOURNALAinda não há avaliações
- Dapa Brief Data (14271)Documento24 páginasDapa Brief Data (14271)Adel SALLAM100% (1)
- Basal Bolus InsulinDMT22009Documento92 páginasBasal Bolus InsulinDMT22009scribdAinda não há avaliações
- Post-Cardiac Arrest Therapeutic Hypothermia Targeted Temperature Manangement (TTM) Quick SheetDocumento3 páginasPost-Cardiac Arrest Therapeutic Hypothermia Targeted Temperature Manangement (TTM) Quick SheetkimberlyAinda não há avaliações
- Cardiovascular Outcomes Trials in Type 2 DiabetesDocumento51 páginasCardiovascular Outcomes Trials in Type 2 Diabetes와라송이100% (1)
- A Randomized, Double-Blind, Controlled Trial Comparing Rifaximin Plus Lactulose With Lactulose Alone in Treatment of Overt Hepatic EncephalopathyDocumento3 páginasA Randomized, Double-Blind, Controlled Trial Comparing Rifaximin Plus Lactulose With Lactulose Alone in Treatment of Overt Hepatic EncephalopathyYunita DAinda não há avaliações
- 1117 FullDocumento29 páginas1117 FullElizabeth IB100% (1)
- Pharmacy PresentationDocumento93 páginasPharmacy PresentationAira Abella100% (1)
- Review: Marcel H A Muskiet, David C Wheeler, Hiddo J L HeerspinkDocumento16 páginasReview: Marcel H A Muskiet, David C Wheeler, Hiddo J L Heerspinkellya theresia100% (1)
- Ultimate Reference DocumentDocumento29 páginasUltimate Reference DocumentShellyza Moledina SajwaniAinda não há avaliações
- Know Common Disease ManagementDocumento14 páginasKnow Common Disease Managementcdx25Ainda não há avaliações
- Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy CREDENCE TrialDocumento29 páginasCanagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy CREDENCE Trialgokulam0075028Ainda não há avaliações
- Klasifikasi Dan Mekanisme ABDocumento8 páginasKlasifikasi Dan Mekanisme ABDeboyjackAinda não há avaliações
- IvabradineDocumento33 páginasIvabradinepashaAinda não há avaliações
- Adult - Pediatric Antibiotic Prescribing Guidelines 2017Documento4 páginasAdult - Pediatric Antibiotic Prescribing Guidelines 2017dremad1974Ainda não há avaliações
- Treatment and Classification of Heart FailureDocumento2 páginasTreatment and Classification of Heart FailureShannon RamsumairAinda não há avaliações
- Outcomes of SGLT2i in diabetic kidney disease: is it all diabetesDocumento29 páginasOutcomes of SGLT2i in diabetic kidney disease: is it all diabetesVaibhav DafaleAinda não há avaliações
- HemodialysisDocumento6 páginasHemodialysisAnonymous 7LI78gu4VDAinda não há avaliações
- Eportfolio SampleDocumento46 páginasEportfolio SampleJolaine ValloAinda não há avaliações
- 2020 Apr Common Treatment OrdersDocumento32 páginas2020 Apr Common Treatment OrdersAlistair LauAinda não há avaliações
- GYNECOLOGY Chief ComplaintsDocumento3 páginasGYNECOLOGY Chief ComplaintsJennifer HerediaAinda não há avaliações
- AIIMS June 2020 DR Siraj Ahmad PDFDocumento4 páginasAIIMS June 2020 DR Siraj Ahmad PDFadiAinda não há avaliações
- Controlled Substances LawsDocumento8 páginasControlled Substances LawsJames Lindon100% (1)
- Medical grading scales and assessment criteriaDocumento17 páginasMedical grading scales and assessment criteriaSerious LeoAinda não há avaliações
- PracticeExam 4 QsDocumento17 páginasPracticeExam 4 QsBehrouz YariAinda não há avaliações
- Internal MedicineDocumento83 páginasInternal MedicineSumbul PAinda não há avaliações
- Mechanism of Action For Each Class of AntiDocumento146 páginasMechanism of Action For Each Class of AntiReynaldo RiveraAinda não há avaliações
- (Warding) Guideline 1 - QCGH-HISTORY - PE - GUIDELINEDocumento4 páginas(Warding) Guideline 1 - QCGH-HISTORY - PE - GUIDELINEHynne Jhea Echavez100% (1)
- HF2019Documento24 páginasHF2019Sima Noviantika100% (2)
- Therapeutic Cooling Protocol for Perinatal AsphyxiaDocumento31 páginasTherapeutic Cooling Protocol for Perinatal AsphyxiaNiraj GuptaAinda não há avaliações
- SGLT2i Beyond Glycemic ControlDocumento55 páginasSGLT2i Beyond Glycemic ControlSwapnaAinda não há avaliações
- ALD WITH ASCITES by VaibhavDocumento22 páginasALD WITH ASCITES by VaibhavSandeep ChakravarthyAinda não há avaliações
- Acute Decompensated Heart FailureDocumento31 páginasAcute Decompensated Heart Failure568563Ainda não há avaliações
- Emergency Drugs: Drug Action Indications Adverse Effects Contraindications Nursing Management Atropine SulfateDocumento15 páginasEmergency Drugs: Drug Action Indications Adverse Effects Contraindications Nursing Management Atropine Sulfate092109Ainda não há avaliações
- Classification of The DrugsDocumento50 páginasClassification of The DrugsGlena SalamAinda não há avaliações
- Critical Care Drugs OverviewDocumento23 páginasCritical Care Drugs OverviewAsri Ernadi100% (1)
- Junior Intern NotesDocumento3 páginasJunior Intern NotesTin SumangaAinda não há avaliações
- 2002 GAO PDMP StudyDocumento27 páginas2002 GAO PDMP StudyKOMU NewsAinda não há avaliações
- Pre-Operative Orders Post-Op Orders (Ga)Documento3 páginasPre-Operative Orders Post-Op Orders (Ga)Alissandra OcampoAinda não há avaliações
- World Preview 2016 Outlook To 2022Documento49 páginasWorld Preview 2016 Outlook To 2022Willy Pérez-Barreto MaturanaAinda não há avaliações
- Medicine Epidemiology (MedicalBooksVN - Com)Documento34 páginasMedicine Epidemiology (MedicalBooksVN - Com)Jonathan AiresAinda não há avaliações
- Physician Order Sheet Format GuideDocumento9 páginasPhysician Order Sheet Format GuideRoland Philip GoAinda não há avaliações
- THURSDAY Salisbury AfsharDocumento39 páginasTHURSDAY Salisbury AfsharNational Press Foundation100% (1)
- Best Practice ProtocolsDocumento46 páginasBest Practice ProtocolsRaigheil LayAinda não há avaliações
- Hypertensive Work Up Age Work Up Ugib Work Up Stroke Work UpDocumento5 páginasHypertensive Work Up Age Work Up Ugib Work Up Stroke Work UpGeraldine Marie SalvoAinda não há avaliações
- OsteoporosisDocumento19 páginasOsteoporosisLasa SiahaanAinda não há avaliações
- Spinal Cord CompressionDocumento4 páginasSpinal Cord Compressionian3yeung-2Ainda não há avaliações
- A Speech On PunctualityDocumento2 páginasA Speech On PunctualityRrhayshelle Ahnne0% (1)
- Drugs To Watch With WARFARINDocumento3 páginasDrugs To Watch With WARFARINRajendra RaiAinda não há avaliações
- Problem-based Approach to Gastroenterology and HepatologyNo EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisAinda não há avaliações
- Chinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Documento11 páginasChinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Reda SoAinda não há avaliações
- CHAPTER 55 - Percutaneous Coronary InterventionDocumento1 páginaCHAPTER 55 - Percutaneous Coronary InterventionReda SoAinda não há avaliações
- Ward Reflection PaperDocumento1 páginaWard Reflection PaperReda SoAinda não há avaliações
- Answer Key-Mitral ValveDocumento6 páginasAnswer Key-Mitral ValveReda SoAinda não há avaliações
- Chapter 32 - Genetic Cardiac ArrythmiasDocumento7 páginasChapter 32 - Genetic Cardiac ArrythmiasReda SoAinda não há avaliações
- Risk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Documento7 páginasRisk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Reda SoAinda não há avaliações
- Braunwald Chapter KeypointersDocumento6 páginasBraunwald Chapter KeypointersReda SoAinda não há avaliações
- CHAPTER 27 - Heart Failure With A Preserved Ejection FractionDocumento15 páginasCHAPTER 27 - Heart Failure With A Preserved Ejection FractionReda SoAinda não há avaliações
- CH 50 - Approach To Patient With Chest PainDocumento1 páginaCH 50 - Approach To Patient With Chest PainReda SoAinda não há avaliações
- Name: - Year LevelDocumento6 páginasName: - Year LevelReda SoAinda não há avaliações
- Mitral Valve Disease QuizDocumento5 páginasMitral Valve Disease QuizReda SoAinda não há avaliações
- Private Ward Admission Census 1Documento6 páginasPrivate Ward Admission Census 1Reda SoAinda não há avaliações
- Evidence-Based Approach to Heart Failure History and Physical ExamDocumento5 páginasEvidence-Based Approach to Heart Failure History and Physical ExamReda SoAinda não há avaliações
- Tilt Table Testing: Name Age/Sex APDocumento1 páginaTilt Table Testing: Name Age/Sex APReda SoAinda não há avaliações
- Coronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Documento3 páginasCoronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Reda SoAinda não há avaliações
- Rapid Response and Cardiac Arrest TeamsDocumento11 páginasRapid Response and Cardiac Arrest TeamsReda SoAinda não há avaliações
- Aortic ExamDocumento3 páginasAortic ExamReda SoAinda não há avaliações
- CHAPTER 61: Diabetes and The Cardiovascular System: Ma. Arnee V. Anico-Tondo, M.D., FPCP (CGH)Documento1 páginaCHAPTER 61: Diabetes and The Cardiovascular System: Ma. Arnee V. Anico-Tondo, M.D., FPCP (CGH)Reda SoAinda não há avaliações
- Coronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Documento3 páginasCoronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Reda SoAinda não há avaliações
- Vascular Conference: JUNE 2018 - MARCH 2019Documento2 páginasVascular Conference: JUNE 2018 - MARCH 2019Reda SoAinda não há avaliações
- Cardiology census and patient detailsDocumento9 páginasCardiology census and patient detailsReda SoAinda não há avaliações
- Heart Institute Team Building April 2019Documento1 páginaHeart Institute Team Building April 2019Reda SoAinda não há avaliações
- Marijuana LegalizationDocumento5 páginasMarijuana LegalizationMatt ImpellusoAinda não há avaliações
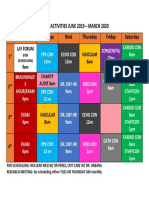
- Daily Activities 2019Documento1 páginaDaily Activities 2019Reda SoAinda não há avaliações
- Tilt Table Testing: Name Age/Sex APDocumento1 páginaTilt Table Testing: Name Age/Sex APReda SoAinda não há avaliações
- Computed Tomography Findings for 8 Cardiovascular PatientsDocumento1 páginaComputed Tomography Findings for 8 Cardiovascular PatientsReda SoAinda não há avaliações
- 2011 PadDocumento19 páginas2011 PadReda SoAinda não há avaliações
- Case Protocol 3Documento5 páginasCase Protocol 3Reda SoAinda não há avaliações
- Case Protocol 3Documento2 páginasCase Protocol 3Reda SoAinda não há avaliações
- Cardiovascular Diseases and Dental CareDocumento73 páginasCardiovascular Diseases and Dental Careasop06Ainda não há avaliações
- ABLS PROVIDER MANUAL 2015 Revisions PDFDocumento133 páginasABLS PROVIDER MANUAL 2015 Revisions PDFBrinaAinda não há avaliações
- Holter SolutionsDocumento4 páginasHolter SolutionsgimenAinda não há avaliações
- Interpretation of Stress TestsDocumento26 páginasInterpretation of Stress TestsHashini VjkmrAinda não há avaliações
- Unit #2 Medical Equipment: BandageDocumento2 páginasUnit #2 Medical Equipment: BandageSahara SaharaAinda não há avaliações
- Case presentationPHCDocumento149 páginasCase presentationPHCChitPerRhosAinda não há avaliações
- Pacemaker ImplantDocumento62 páginasPacemaker Implantadins100% (1)
- ECG InterpretationDocumento81 páginasECG Interpretationd.ramadhan100% (3)
- Eating Disorder TeenagerDocumento47 páginasEating Disorder TeenagerWolfy D HaroldAinda não há avaliações
- Bradycardia and TachycardiaDocumento66 páginasBradycardia and TachycardiaKarissaAinda não há avaliações
- Prosim 8: Technical DataDocumento12 páginasProsim 8: Technical DataAqsa AqsaAinda não há avaliações
- Ehz 467Documento65 páginasEhz 467Coy Calapatia-TorresAinda não há avaliações
- Main Abbrevations 12Documento37 páginasMain Abbrevations 12niksomiAinda não há avaliações
- Eng BSM 3000 SpecsDocumento20 páginasEng BSM 3000 Specsamirali.bme4527Ainda não há avaliações
- Defibrillator Sync TestingDocumento4 páginasDefibrillator Sync TestingYahya SalemAinda não há avaliações
- ACC/AHA Guidelines For Implantation of Cardiac Pacemakers and Antiarrhythmia Devices: Executive SummaryDocumento12 páginasACC/AHA Guidelines For Implantation of Cardiac Pacemakers and Antiarrhythmia Devices: Executive SummarysmtandelAinda não há avaliações
- Conduction System of Heart and Temporary PacemakerDocumento23 páginasConduction System of Heart and Temporary Pacemakersmruti prakash SahuAinda não há avaliações
- Case Study on Pacemakers: How They Work and Their BenefitsDocumento6 páginasCase Study on Pacemakers: How They Work and Their BenefitsBalamuruganAinda não há avaliações
- ECG Study GuideDocumento70 páginasECG Study GuideFatima Chrystelle NuñalAinda não há avaliações
- Intraoperative ArrhythmiasDocumento22 páginasIntraoperative ArrhythmiasJosephAinda não há avaliações
- Wearable Bio Sensors Og Report AneesDocumento22 páginasWearable Bio Sensors Og Report AneesSufail AAinda não há avaliações
- BIOLOGY PROJECT (Class 12)Documento21 páginasBIOLOGY PROJECT (Class 12)Manoghna MaheshAinda não há avaliações
- National Patient Safety GoalsDocumento5 páginasNational Patient Safety GoalsMariam AbedAinda não há avaliações
- Paroxysmal Supraventricular Tachycardia: Pathophysiology, Diagnosis, and ManagementDocumento8 páginasParoxysmal Supraventricular Tachycardia: Pathophysiology, Diagnosis, and ManagementLaurensia Sherly SusiloAinda não há avaliações
- LA County Treatment Protocols 2018-12-01Documento371 páginasLA County Treatment Protocols 2018-12-01Anonymous gTXqJVAmAinda não há avaliações