Você também pode gostar
- Basoglu 2010Documento7 páginasBasoglu 2010Cansu UnsalAinda não há avaliações
- A Placebo-Controlled Pilot Study of Adjunctive OlanzapineDocumento6 páginasA Placebo-Controlled Pilot Study of Adjunctive OlanzapineloloasbAinda não há avaliações
- Cap 2009 0098Documento8 páginasCap 2009 0098jacopo pruccoliAinda não há avaliações
- Topiramate For Prevention of Olanzapine Associated Weight Gai - 2010 - SchizophrDocumento6 páginasTopiramate For Prevention of Olanzapine Associated Weight Gai - 2010 - SchizophrSol ContrerasAinda não há avaliações
- Armodafinil in Binge Eating Disorder A RandomizedDocumento7 páginasArmodafinil in Binge Eating Disorder A RandomizedQuel PaivaAinda não há avaliações
- Outcomes of Obese, Clozapine-Treated Inpatients With Schizophrenia Placed On A Six-Month Diet and Physical Activity ProgramDocumento7 páginasOutcomes of Obese, Clozapine-Treated Inpatients With Schizophrenia Placed On A Six-Month Diet and Physical Activity ProgramnajibrendraAinda não há avaliações
- Jurnal 5Documento7 páginasJurnal 5nurindahwarAinda não há avaliações
- Revision Antipsicoticos Alteraciones Metabolicas OJO Imagenes 2019Documento10 páginasRevision Antipsicoticos Alteraciones Metabolicas OJO Imagenes 2019siralkAinda não há avaliações
- Long Term Oxandrone TherapyDocumento17 páginasLong Term Oxandrone TherapynikitagustiAinda não há avaliações
- Lee 2012Documento6 páginasLee 2012jhomarlaiAinda não há avaliações
- Effects of Auricular Acupressure On Obesity in Adolescents With ObesityDocumento7 páginasEffects of Auricular Acupressure On Obesity in Adolescents With ObesityMaurocoAinda não há avaliações
- Obesity, Antioxidants and Negative SymptomDocumento6 páginasObesity, Antioxidants and Negative SymptomsiralkAinda não há avaliações
- Appi Ajp 2008 07121900Documento8 páginasAppi Ajp 2008 07121900jacopo pruccoliAinda não há avaliações
- Motivation To Eat and Not To Eat - The Psycho-Biological Conflict in Anorexia NervosaDocumento6 páginasMotivation To Eat and Not To Eat - The Psycho-Biological Conflict in Anorexia NervosaCristina PaizAinda não há avaliações
- The Investigation of Leptin and Hypothalamic Neuropeptides Role in First Attack Psychotic Male Patients: Olanzapine MonotherapyDocumento7 páginasThe Investigation of Leptin and Hypothalamic Neuropeptides Role in First Attack Psychotic Male Patients: Olanzapine MonotherapyCansu UnsalAinda não há avaliações
- CCR3 8 2827Documento8 páginasCCR3 8 2827jacopo pruccoliAinda não há avaliações
- Nihms 1669289Documento8 páginasNihms 1669289triska antonyAinda não há avaliações
- Engl2005 Article ToMackinPWatkinsonHMYoungAH200Documento2 páginasEngl2005 Article ToMackinPWatkinsonHMYoungAH200Hesbon MomanyiAinda não há avaliações
- Schizophrenia Research: Man Wang, Jian-Hua Tong, Gang Zhu, Guang-Ming Liang, Hong-Fei Yan, Xiu-Zhen WangDocumento4 páginasSchizophrenia Research: Man Wang, Jian-Hua Tong, Gang Zhu, Guang-Ming Liang, Hong-Fei Yan, Xiu-Zhen WangSol ContrerasAinda não há avaliações
- Hisayuki - AcupunctureDocumento7 páginasHisayuki - AcupunctureYosfikriansyahYosfiqarAinda não há avaliações
- 12 - Methapatara2011Documento7 páginas12 - Methapatara2011Sergio Machado NeurocientistaAinda não há avaliações
- Qigong and Blood Pressure CholesterolDocumento12 páginasQigong and Blood Pressure CholesterolLaili ZikriyaAinda não há avaliações
- Complementary and Alternative Medical Lab Testing Part 18: PsychiatryNo EverandComplementary and Alternative Medical Lab Testing Part 18: PsychiatryNota: 5 de 5 estrelas5/5 (1)
- Anorexia NervosaDocumento4 páginasAnorexia NervosaFarida RahmaAinda não há avaliações
- Why Is Premixed Insulin The Preferred Insulin? Novel Answers To A Decade-Old QuestionDocumento3 páginasWhy Is Premixed Insulin The Preferred Insulin? Novel Answers To A Decade-Old QuestionDanielShenfieldAinda não há avaliações
- Anorexia Nervosa - Aetiology, Assessment, and TreatmentDocumento13 páginasAnorexia Nervosa - Aetiology, Assessment, and TreatmentDouglas SantosAinda não há avaliações
- 10 1089@cap 2016 0178Documento2 páginas10 1089@cap 2016 0178Maria Helena Pedraza MAinda não há avaliações
- OlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Documento5 páginasOlanzapineEarlyPredictorsWeightGainBipolarDisorder LIPKOVICH JClinPsychopharm2006Leslie CitromeAinda não há avaliações
- J Cachexia Sarcopenia Muscle - 2023 - Aprahamian - Anorexia of Aging An International Assessment of HealthcareDocumento14 páginasJ Cachexia Sarcopenia Muscle - 2023 - Aprahamian - Anorexia of Aging An International Assessment of HealthcareMauricio LorcaAinda não há avaliações
- Original Paper: World Nutrition JournalDocumento6 páginasOriginal Paper: World Nutrition JournalSaptawati BardosonoAinda não há avaliações
- Huang2021 Article APotentialProbioticBacteriumFoDocumento11 páginasHuang2021 Article APotentialProbioticBacteriumFoCleisson SchosslerAinda não há avaliações
- Effectiveness of Olanzapine in The Treaatment of AnorexiaDocumento6 páginasEffectiveness of Olanzapine in The Treaatment of AnorexiaBetzaida Maritza Vela TrujilloAinda não há avaliações
- Abstracts Clinical Nutrition ESPEN 40 (2020) 412 E690Documento2 páginasAbstracts Clinical Nutrition ESPEN 40 (2020) 412 E690yafanitaizzatiAinda não há avaliações
- Olanzapin and Risperidone Terhadap AppetiteDocumento5 páginasOlanzapin and Risperidone Terhadap AppetiteDewi NofiantiAinda não há avaliações
- 6 Cheng2017Documento7 páginas6 Cheng2017Sergio Machado NeurocientistaAinda não há avaliações
- Aigner WFSBP Guidelines Eating Disorder World J Biol Psychia 11Documento44 páginasAigner WFSBP Guidelines Eating Disorder World J Biol Psychia 11scabrera_scribdAinda não há avaliações
- Antiepileptic Drugs Montherapy and Hematolgic, Japin 2019Documento13 páginasAntiepileptic Drugs Montherapy and Hematolgic, Japin 2019Mohammed Abdullah AlqaadAinda não há avaliações
- Nonpharmacological Treatment of EpilepsyDocumento6 páginasNonpharmacological Treatment of Epilepsynguyen truongAinda não há avaliações
- Article 2 CDocumento6 páginasArticle 2 Cfy fyAinda não há avaliações
- Bestpracticesinthe Managementofoverweight Andobesity: Beverly G. Tchang,, Katherine H. Saunders,, Leon I. IgelDocumento26 páginasBestpracticesinthe Managementofoverweight Andobesity: Beverly G. Tchang,, Katherine H. Saunders,, Leon I. Igelvallabhaneni rajeshAinda não há avaliações
- Randomized Controlled Trial of Yoga and Exercise in Multiple SclerosisDocumento8 páginasRandomized Controlled Trial of Yoga and Exercise in Multiple Sclerosisfrogsmasher420Ainda não há avaliações
- 1 s2.0 S0165032718305895 MainDocumento8 páginas1 s2.0 S0165032718305895 MainMurizzaldi YussufAinda não há avaliações
- Jurnal 2Documento7 páginasJurnal 2dewi pspta sriAinda não há avaliações
- Influence of Psychopathology and Metabolic Parameters en Primeros Episodios PsicoticosDocumento7 páginasInfluence of Psychopathology and Metabolic Parameters en Primeros Episodios PsicoticossiralkAinda não há avaliações
- Akyurek 2006Documento4 páginasAkyurek 2006Jean Carlo Siqueira de OliveiraAinda não há avaliações
- Decrease in Self-Efficacy For Exercise at 12 Weeks After Exercise Education in Diabetic PatientsDocumento8 páginasDecrease in Self-Efficacy For Exercise at 12 Weeks After Exercise Education in Diabetic PatientsFiskha WihanarniAinda não há avaliações
- Journal of Yoga & Physical Therapy: Impact of A 10 Minute Seated Yoga Practice in The Management of DiabetesDocumento3 páginasJournal of Yoga & Physical Therapy: Impact of A 10 Minute Seated Yoga Practice in The Management of Diabetessankapalrutik10Ainda não há avaliações
- Decreased Levels of Spexin - Case Control StudyDocumento7 páginasDecreased Levels of Spexin - Case Control StudyvaskoreAinda não há avaliações
- Anorexia Nervosa What Has Changed in The State of Knowledge About Nutritional RehabilitationDocumento13 páginasAnorexia Nervosa What Has Changed in The State of Knowledge About Nutritional RehabilitationAlejandro Flores VelascoAinda não há avaliações
- Danhauer 2017 Reviewof Yoga Therapy During Cancer TreatmentDocumento24 páginasDanhauer 2017 Reviewof Yoga Therapy During Cancer TreatmentfitranoenoeAinda não há avaliações
- Intermittent Fasting and Obesity-Related Health OutcomesDocumento12 páginasIntermittent Fasting and Obesity-Related Health Outcomesthe.bracelet.down.underAinda não há avaliações
- Hormonal ImbalanceDocumento3 páginasHormonal ImbalanceAkshaya SairamAinda não há avaliações
- Combined Caloric Restriction and Exercise Provides Greater Metabolic andDocumento10 páginasCombined Caloric Restriction and Exercise Provides Greater Metabolic andyhenti widjayantiAinda não há avaliações
- Pharmacologic and Nonpharmacologic Strategies For Weight Gain and Metabolic Disturbance in Patients Treated With Antipsychotic MedicationsDocumento10 páginasPharmacologic and Nonpharmacologic Strategies For Weight Gain and Metabolic Disturbance in Patients Treated With Antipsychotic MedicationsiceberghoneyAinda não há avaliações
- MetadecDocumento18 páginasMetadecRajpal Singh KochharAinda não há avaliações
- Cancer Treatment and Research Communications: Timotius Ivan Hariyanto, Andree KurniawanDocumento10 páginasCancer Treatment and Research Communications: Timotius Ivan Hariyanto, Andree Kurniawandevin mahendikaAinda não há avaliações
- Relationship Between Job Stress and Functional Dyspepsia in Display Manufacturing Sector Workers: A Cross-Sectional StudyDocumento9 páginasRelationship Between Job Stress and Functional Dyspepsia in Display Manufacturing Sector Workers: A Cross-Sectional StudyZilfiah LAinda não há avaliações
- The Role of Psychotropic Medications in The ManagementDocumento24 páginasThe Role of Psychotropic Medications in The ManagementloloasbAinda não há avaliações
- The Prevention and Cure Effects of Aspirin Eugenol Ester On Hyperlipidemia and Its MetabonomicsDocumento108 páginasThe Prevention and Cure Effects of Aspirin Eugenol Ester On Hyperlipidemia and Its MetabonomicsKavisa GhoshAinda não há avaliações
- AsthmaDocumento55 páginasAsthmaAlessandra CruzAinda não há avaliações
- Infantile Hypertrophic Pyloric StenosisDocumento25 páginasInfantile Hypertrophic Pyloric StenosisPirapong Invalueable KunokAinda não há avaliações
- NCP Disturbed Body ImageDocumento5 páginasNCP Disturbed Body ImageAira AlaroAinda não há avaliações
- Crash Cart Check ListDocumento2 páginasCrash Cart Check Listkim reyesAinda não há avaliações
- Albuterol, Accuneb Drug CardDocumento2 páginasAlbuterol, Accuneb Drug Carddnw876Ainda não há avaliações
- Introduction To DSM 5 2Documento61 páginasIntroduction To DSM 5 2denfan100% (1)
- Ever Increasing Faith Magazine - Issue 3 - 2013Documento32 páginasEver Increasing Faith Magazine - Issue 3 - 2013jsuccessAinda não há avaliações
- 180-Day Exclusivity TrackerDocumento4.005 páginas180-Day Exclusivity Trackershah777Ainda não há avaliações
- Psychological DisordersDocumento50 páginasPsychological DisordersAmirullah ZulkifliAinda não há avaliações
- Calf Protocols Ver4Documento6 páginasCalf Protocols Ver4Sadam Irshad100% (1)
- CBE - Platelet AbnormalitiesDocumento3 páginasCBE - Platelet AbnormalitiesRuxandra MesarosAinda não há avaliações
- Kimberli Case StudyDocumento4 páginasKimberli Case StudyLLLJJJ100% (3)
- Understanding Psychological Testing and AssessmentDocumento3 páginasUnderstanding Psychological Testing and AssessmentdevAinda não há avaliações
- Boala Obsesiv CompulsivaDocumento134 páginasBoala Obsesiv CompulsivalumyciunguAinda não há avaliações
- Fluid and Electrolyte Therapy, Calculation of Fluids and Its AdministrationDocumento11 páginasFluid and Electrolyte Therapy, Calculation of Fluids and Its AdministrationAnusha Verghese100% (2)
- Label ObatDocumento31 páginasLabel ObatAndiTenriBayangAinda não há avaliações
- Dr. Smith's ECG Blog - "Shark Fin" - A Deadly ECG Sign That You Must Know! PDFDocumento7 páginasDr. Smith's ECG Blog - "Shark Fin" - A Deadly ECG Sign That You Must Know! PDFZACHARIAH MANKIRAinda não há avaliações
- Association Between Psychotherapy Content and Clinical Outcomes Using Deep LearningDocumento9 páginasAssociation Between Psychotherapy Content and Clinical Outcomes Using Deep LearningfuturistzgAinda não há avaliações
- Chapter Outline Overview of Adler's Individual PsychologyDocumento2 páginasChapter Outline Overview of Adler's Individual PsychologyNur MNAinda não há avaliações
- Amelogenesis Imperfecta Treatment Case ReviewDocumento7 páginasAmelogenesis Imperfecta Treatment Case ReviewGeraldo LaurusAinda não há avaliações
- Food Cures For Spleen Qi Deficiency - Chinese MedicineDocumento9 páginasFood Cures For Spleen Qi Deficiency - Chinese MedicineJ.J.Ainda não há avaliações
- Infusion Site Selection and Infusion Set ChangeDocumento8 páginasInfusion Site Selection and Infusion Set ChangegaridanAinda não há avaliações
- Jagl Ev4 McmoliiDocumento7 páginasJagl Ev4 McmoliiJasson GaunaAinda não há avaliações
- Level 2 BookDocumento176 páginasLevel 2 BookPriyesh BargalAinda não há avaliações
- SCLC A Cancer PowerpointDocumento7 páginasSCLC A Cancer Powerpointapi-353368377Ainda não há avaliações
- Bates Method - Wikipedia, The Free EncyclopediaDocumento14 páginasBates Method - Wikipedia, The Free EncyclopediaVd Vivek SharmaAinda não há avaliações
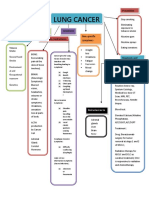
- Concept Map LungDocumento1 páginaConcept Map LungThea Eya FayeAinda não há avaliações
- Chakra Therapy - Balancing ..Documento3 páginasChakra Therapy - Balancing ..ankita_asthanAinda não há avaliações
- Hepatitis C: by DR Faiza SamadDocumento44 páginasHepatitis C: by DR Faiza SamadMuhammad MakkiAinda não há avaliações
- Administration of MedicationDocumento18 páginasAdministration of MedicationThilaga RamAinda não há avaliações