Você também pode gostar
- MKSAP Normal Lab ValuesDocumento2 páginasMKSAP Normal Lab Valuesdzhao09Ainda não há avaliações
- IDSA - Guía de Infección Asociada A Catéter VenosoDocumento45 páginasIDSA - Guía de Infección Asociada A Catéter Venosoivonne micoltaAinda não há avaliações
- Epidemiology - AMBOSSDocumento13 páginasEpidemiology - AMBOSSFlowerAinda não há avaliações
- Dual Antiplatelet Therapy Vs Alteplase For Patients With Minor NondisablingDocumento10 páginasDual Antiplatelet Therapy Vs Alteplase For Patients With Minor Nondisablingbetongo Bultus Ocultus XVAinda não há avaliações
- II EXAMEN DEPARTAMENTALSR LDocumento8 páginasII EXAMEN DEPARTAMENTALSR LPaloma JGAinda não há avaliações
- Caso MicroDocumento36 páginasCaso MicroFernando Román RubioAinda não há avaliações
- Nejmra 2000348Documento16 páginasNejmra 2000348Mathew McCarthyAinda não há avaliações
- Antiarritmicos PPT FinalDocumento81 páginasAntiarritmicos PPT FinalCarolina González RiveraAinda não há avaliações
- Manual Cardiologia y Cirugia CardiovascularDocumento84 páginasManual Cardiologia y Cirugia CardiovascularAna Sylvia AguilarAinda não há avaliações
- Clinical States of Cirrhosis and Competing RisksDocumento14 páginasClinical States of Cirrhosis and Competing RisksmaryAinda não há avaliações
- Pulmonary HypertensionDocumento20 páginasPulmonary Hypertensionyelsinosmin romeroalvaradoAinda não há avaliações
- Casos Clinicos de Ginecologia y Obstetricia Clinical Cases of Gynecology and Obstetrics Spanish Edition by Roberto Matorras WeinigJose Remohi PDFDocumento5 páginasCasos Clinicos de Ginecologia y Obstetricia Clinical Cases of Gynecology and Obstetrics Spanish Edition by Roberto Matorras WeinigJose Remohi PDFV Hugo J ChoqueAinda não há avaliações
- Acid-Base, Fluids, and Electrolytes Made Ridiculously SimpleDocumento2 páginasAcid-Base, Fluids, and Electrolytes Made Ridiculously Simpledennis georgeAinda não há avaliações
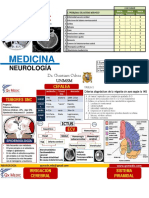
- Medicina 4 Neuro Neumo PDFDocumento19 páginasMedicina 4 Neuro Neumo PDFKarol M MChAinda não há avaliações
- Guía Basada en La Evidencia. Diagnóstico Y Manejo Del Síndrome de Guillain-Barré en Diez PasosDocumento20 páginasGuía Basada en La Evidencia. Diagnóstico Y Manejo Del Síndrome de Guillain-Barré en Diez PasosMichelle CortesAinda não há avaliações
- Adenocarcinoma PulmonarDocumento75 páginasAdenocarcinoma PulmonarLigia Micaela García XitamulAinda não há avaliações
- Liquidos y Electrolitos en CirugiaDocumento161 páginasLiquidos y Electrolitos en CirugiaFrancis AbdalaAinda não há avaliações
- Antiphospholipid Antibody Syndrome The.2 PDFDocumento5 páginasAntiphospholipid Antibody Syndrome The.2 PDFJunita Nelly Esther JosephAinda não há avaliações
- Semiologia Renal Argente Alvarez 2a EdDocumento135 páginasSemiologia Renal Argente Alvarez 2a EdNancy Mac Lean Balboa100% (1)
- Misión: Licenciatura en MedicinaDocumento7 páginasMisión: Licenciatura en MedicinaMonserrat DiazAinda não há avaliações
- Cto Endocrinologia Metabolismo y Nutricion Mexico Cto 1 EdDocumento179 páginasCto Endocrinologia Metabolismo y Nutricion Mexico Cto 1 EdJoel GutierrezAinda não há avaliações
- Neutropenic Fever: Dr. Meral SönmezoğluDocumento67 páginasNeutropenic Fever: Dr. Meral SönmezoğluOguzcan KinikogluAinda não há avaliações
- Jama Mederos 2021 RV 200014 1655494806.72368Documento9 páginasJama Mederos 2021 RV 200014 1655494806.72368Soni CollinAinda não há avaliações
- Axenfeld-Rieger Syndrome (ARS)Documento14 páginasAxenfeld-Rieger Syndrome (ARS)CESAR GERARDO REYES MORENO100% (1)
- HSA ContinuunDocumento35 páginasHSA ContinuunJose DavidAinda não há avaliações
- INFECTOLOGIADocumento144 páginasINFECTOLOGIAYads MoAinda não há avaliações
- Enarm Casos Clinicos en Ingles PDFDocumento101 páginasEnarm Casos Clinicos en Ingles PDFLuis Angel Amezcua100% (1)
- Manual Resimed Oftalmologia PDFDocumento41 páginasManual Resimed Oftalmologia PDFLuz Carola Perez ZelaezAinda não há avaliações
- Atypical Exanthems in Children PDFDocumento30 páginasAtypical Exanthems in Children PDFrosela_obandoAinda não há avaliações
- Surviving Sepsis Campaign 2021 Guidelines Infographic Vasoactive AgentDocumento1 páginaSurviving Sepsis Campaign 2021 Guidelines Infographic Vasoactive AgentAnsel AriaAinda não há avaliações
- Sepsis Neonatal LecturaDocumento32 páginasSepsis Neonatal LecturaValen CadenaAinda não há avaliações
- Tep Nejm 2022Documento13 páginasTep Nejm 2022Jorge CastilloAinda não há avaliações
- Anti-GBM Disease: (Goodpasture Syndrome)Documento35 páginasAnti-GBM Disease: (Goodpasture Syndrome)pashaAinda não há avaliações
- Exam 2 Study Guide 2018Documento21 páginasExam 2 Study Guide 2018EvanAinda não há avaliações
- 9.pneumonia 1 Nov '19Documento62 páginas9.pneumonia 1 Nov '19Arleen MatincaAinda não há avaliações
- MICRO2015 - Prelims To Finals Theo ReviewerDocumento7 páginasMICRO2015 - Prelims To Finals Theo ReviewerAndrassy Twinkle AlineaAinda não há avaliações
- Bacte MnemonicsDocumento10 páginasBacte MnemonicsIan Leo SantosAinda não há avaliações
- Bacterio BilityDocumento8 páginasBacterio BilityAbdul Rehman SafdarAinda não há avaliações
- MBL 1 Bacterial PneumoniaDocumento5 páginasMBL 1 Bacterial PneumoniaFadhlina OmarAinda não há avaliações
- Pneumonia - Spread SheetDocumento1 páginaPneumonia - Spread SheetRobin KeaneAinda não há avaliações
- Gram Negative Video LectureDocumento50 páginasGram Negative Video LectureAnna CrisAinda não há avaliações
- Microbiology MnemonicsDocumento5 páginasMicrobiology MnemonicsFritzel SusbillaAinda não há avaliações
- Microbiology PinkDocumento3 páginasMicrobiology PinkBenjamin GaliaAinda não há avaliações
- Bacterial PneumoniaDocumento4 páginasBacterial PneumoniaPabinaAinda não há avaliações
- The Lower Respiratory Tract InfectionsDocumento19 páginasThe Lower Respiratory Tract Infectionshibasirag22Ainda não há avaliações
- Cns Infections MbbsDocumento40 páginasCns Infections MbbsSaurabh SharmaAinda não há avaliações
- Pulmonology 5 Lung InfectionsDocumento6 páginasPulmonology 5 Lung InfectionsBenjamin NgAinda não há avaliações
- Blastomycosis Mucomycosis Sialolithiasis Sialosis Halitosis HPVDocumento4 páginasBlastomycosis Mucomycosis Sialolithiasis Sialosis Halitosis HPVAl SyarfinaAinda não há avaliações
- Pneumonia II MicrobesDocumento15 páginasPneumonia II MicrobespuniariAinda não há avaliações
- Microbial Aspect of Respiratory TrackDocumento23 páginasMicrobial Aspect of Respiratory TrackNovi AdriAinda não há avaliações
- Neisse RiaDocumento3 páginasNeisse RiaJanelle GarciaAinda não há avaliações
- Legion EllaDocumento2 páginasLegion EllaJacklyn M. oAinda não há avaliações
- VIRUSDocumento7 páginasVIRUSHet KhokharAinda não há avaliações
- Important Terms - Tropical InfectionDocumento8 páginasImportant Terms - Tropical InfectionTimothy JordanAinda não há avaliações
- PARA - B. Hominis - PsuedomonasDocumento27 páginasPARA - B. Hominis - PsuedomonasMary ChristelleAinda não há avaliações
- Harrison ManuallDocumento105 páginasHarrison Manuallale maril100% (1)
- Pneumonia: DEFINITION: Inflammation of Lung Parenchyma With Involvement of The Alveoli andDocumento10 páginasPneumonia: DEFINITION: Inflammation of Lung Parenchyma With Involvement of The Alveoli andYogesh ValaAinda não há avaliações
- Flash Notes Billie-GeneticsDocumento29 páginasFlash Notes Billie-GeneticsschxzerrydawnAinda não há avaliações
- Chronic Granulomatous Disease 01.23.2019Documento10 páginasChronic Granulomatous Disease 01.23.2019Emily EresumaAinda não há avaliações
- Communicable Disease Nursing BulletsDocumento1 páginaCommunicable Disease Nursing BulletsFaithy HeyAinda não há avaliações
- Antibiotic PolicyDocumento4 páginasAntibiotic PolicyAchmad Faiz SulaimanAinda não há avaliações
- Eclipse 50 EnglishDocumento5 páginasEclipse 50 EnglishVeroniqueroAinda não há avaliações
- Cefuroxime Drug StudyDocumento2 páginasCefuroxime Drug Studymilkv93% (15)
- Anti-Acne Activity of Garcinia Mangostana L.: A ReviewDocumento4 páginasAnti-Acne Activity of Garcinia Mangostana L.: A ReviewifaAinda não há avaliações
- Drug Worksheet - Answers-4Documento3 páginasDrug Worksheet - Answers-4sirnAinda não há avaliações
- Treatment of Humans With Colloidal Silver CompositionDocumento17 páginasTreatment of Humans With Colloidal Silver CompositionkwagAinda não há avaliações
- Pseudomonas AeruginosaDocumento6 páginasPseudomonas AeruginosaMAinda não há avaliações
- Minimal Inhibitory Concentration TestDocumento26 páginasMinimal Inhibitory Concentration TestZandhika Alfi PratamaAinda não há avaliações
- And Antibacterial Resistance: Pseudomonas Aeruginosa: Burn Infection, TreatmentDocumento10 páginasAnd Antibacterial Resistance: Pseudomonas Aeruginosa: Burn Infection, TreatmentnurelisabayuAinda não há avaliações
- A-BART DatasheetDocumento2 páginasA-BART DatasheetIan GibbsAinda não há avaliações
- AntibiotikDocumento10 páginasAntibiotikGeubrina FitrianandaAinda não há avaliações
- Alternative Approaches To Prevent Flu by Dr. Gary NullDocumento13 páginasAlternative Approaches To Prevent Flu by Dr. Gary NullGary NullAinda não há avaliações
- Journal Reading - HordeolumDocumento20 páginasJournal Reading - HordeolumsnylstlAinda não há avaliações
- (Family Medicine) : Dr. Sandip Ganesh PatilDocumento38 páginas(Family Medicine) : Dr. Sandip Ganesh PatilSandip PatilAinda não há avaliações
- Direct Comparison of Antimicrobial SusceptibilityDocumento5 páginasDirect Comparison of Antimicrobial SusceptibilityRoela GeeAinda não há avaliações
- Antibiotic Cross-Sensitivity ChartDocumento1 páginaAntibiotic Cross-Sensitivity ChartChing JuAinda não há avaliações
- AsdassdadDocumento78 páginasAsdassdadLucya PutriAinda não há avaliações
- S C I e N C e SDocumento7 páginasS C I e N C e SEdy TansilAinda não há avaliações
- Dr. Hatem Elgohary Lecturer of General Surgery MD, MrcsDocumento24 páginasDr. Hatem Elgohary Lecturer of General Surgery MD, MrcswinceAinda não há avaliações
- Sr. No. Product Name Packing-All Are Alu-Pvc Blisterfor Tab Cap - For Syrup Pet BottleDocumento2 páginasSr. No. Product Name Packing-All Are Alu-Pvc Blisterfor Tab Cap - For Syrup Pet Bottlesanjay_gawaliAinda não há avaliações
- Audit Penggunaan Aantibiotik Secara Kuantitatif & Kualitatif PDFDocumento9 páginasAudit Penggunaan Aantibiotik Secara Kuantitatif & Kualitatif PDFabd. rahim mubarakAinda não há avaliações
- CHAPTERS1 To 5Documento22 páginasCHAPTERS1 To 5laehaaaa50% (2)
- DSP 15-12-23Documento36 páginasDSP 15-12-23Fu'ad ParkhaniAinda não há avaliações
- Clinical Tuberculosis Multiresitent PDFDocumento10 páginasClinical Tuberculosis Multiresitent PDFsofydianiAinda não há avaliações
- Tugas Praktek Spesialite Iv - Vii (Kel 1)Documento6 páginasTugas Praktek Spesialite Iv - Vii (Kel 1)agustinus randa100% (1)
- EDS Complete NotesDocumento71 páginasEDS Complete NoteseverrainnyAinda não há avaliações
- Acute Bronchitis Chronic Bronchitis: PathophysiologyDocumento2 páginasAcute Bronchitis Chronic Bronchitis: PathophysiologyHarimunsyi Anugerah PratamaAinda não há avaliações
- Study of Drug Resistance in Bacteria Using AntibiotiDocumento10 páginasStudy of Drug Resistance in Bacteria Using AntibiotiAshwin Rockzz75% (4)
- Adhatoda VasicaDocumento10 páginasAdhatoda VasicaMohan PalanisamiAinda não há avaliações
- Lincosamides (Pharmacology of Antibiotics) - Group 6 PresentationDocumento19 páginasLincosamides (Pharmacology of Antibiotics) - Group 6 PresentationGelmark OlivaresAinda não há avaliações