Você também pode gostar
- TROMBOCITOSISDocumento7 páginasTROMBOCITOSISYhajairaAlirivAinda não há avaliações
- EmailserviciosDocumento5 páginasEmailserviciosLoreAinda não há avaliações
- Principios de Bioseguridad PDFDocumento9 páginasPrincipios de Bioseguridad PDFNicoleAinda não há avaliações
- Universidad de San Carlos de Guatemala Facultad de Ciencias MédicasDocumento73 páginasUniversidad de San Carlos de Guatemala Facultad de Ciencias MédicasDaylin Fuente ReyesAinda não há avaliações
- CefaleaDocumento45 páginasCefaleaYahoska Belen Castillo GutierrezAinda não há avaliações
- Wa0011.Documento11 páginasWa0011.Imanol PlasenciaAinda não há avaliações
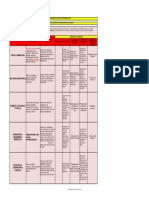
- Matriz de Jerarquizacion de Los Riesgos HigienicosDocumento1 páginaMatriz de Jerarquizacion de Los Riesgos HigienicosHUGO FLOREZ RANGELAinda não há avaliações
- Plan Covid-Corregido 2Documento27 páginasPlan Covid-Corregido 2Martin EscalanteAinda não há avaliações
- 01 02 Introducción A La Biología 2022-2-1Documento17 páginas01 02 Introducción A La Biología 2022-2-1Paula BeltranAinda não há avaliações
- Intubación Bronquial SelectivaDocumento10 páginasIntubación Bronquial SelectivaEduardo Mercado Castro100% (1)
- Casos Clínicos de Pie Diabético Tratado Con HomeopatíaDocumento2 páginasCasos Clínicos de Pie Diabético Tratado Con HomeopatíaKaren Koquito Ferrer Aquino100% (3)
- Ebola VirusDocumento6 páginasEbola VirusrodrigoAinda não há avaliações
- Pepper Mild Mottle Virus (PMMV) : Guía de Síntomas y Daños Del Virus Del Moteado Suave Del PimientoDocumento8 páginasPepper Mild Mottle Virus (PMMV) : Guía de Síntomas y Daños Del Virus Del Moteado Suave Del PimientoSheila Aguilar PardoAinda não há avaliações
- Tratado de Alergología - Antonio Peláez Hernández - Tomos I y IIDocumento1.656 páginasTratado de Alergología - Antonio Peláez Hernández - Tomos I y IIduartelaraferAinda não há avaliações
- Test de Provocacion Con Aspirina PDFDocumento16 páginasTest de Provocacion Con Aspirina PDFRonald CastañoAinda não há avaliações
- Caracteristicas de La Enfermedad Del Adulto MayorDocumento44 páginasCaracteristicas de La Enfermedad Del Adulto MayorRosarioMocarroAinda não há avaliações
- Cambios Sicologicos EmbarazoDocumento13 páginasCambios Sicologicos EmbarazoElyabeth lozadaAinda não há avaliações
- Or To MolecularDocumento236 páginasOr To MolecularLuis Armando Buenaventura100% (1)
- Manual Bundle CocemiDocumento32 páginasManual Bundle CocemiSusan espinoza ulloaAinda não há avaliações
- Directorio UnidadesmedicasDocumento462 páginasDirectorio UnidadesmedicasmenromarAinda não há avaliações
- Ciencia y Tecnologia en Enfermedades RespiratoriasDocumento6 páginasCiencia y Tecnologia en Enfermedades RespiratoriasConsultoria De Tecnologia LMAinda não há avaliações
- Enfermedades en Las Aves FinalDocumento19 páginasEnfermedades en Las Aves FinalROSA STEFANY CHICO ZAMBRANOAinda não há avaliações
- BENLLOCH LÓPEZ María Cruz, UREÑA UREÑA Yolanda, PUIGDENGOLAS ROSAS, Salvador 2015. Conceptos Básicos Sobre Seguridad y Salud en El TrabajoDocumento15 páginasBENLLOCH LÓPEZ María Cruz, UREÑA UREÑA Yolanda, PUIGDENGOLAS ROSAS, Salvador 2015. Conceptos Básicos Sobre Seguridad y Salud en El TrabajoOCHA OCHAAinda não há avaliações
- Trastornos HemodinámicosDocumento2 páginasTrastornos HemodinámicosAnaí MendozaAinda não há avaliações
- AutomedicaciónDocumento25 páginasAutomedicaciónJuan Wilhelm Soriano Villafuerte100% (1)
- Procedimiento Examenes Medicos OcupacionalesDocumento13 páginasProcedimiento Examenes Medicos OcupacionalesDiego PolancoAinda não há avaliações
- Historia Natural de La EnfermedadDocumento1 páginaHistoria Natural de La EnfermedadDulce SandovalAinda não há avaliações
- Polifarmacia FinalDocumento20 páginasPolifarmacia FinalDaniel ÁlvarezAinda não há avaliações
- Breviario EpidemiologiaDocumento3 páginasBreviario EpidemiologiaAisha RodriguezAinda não há avaliações
- Bronquiectasias en NiñosDocumento40 páginasBronquiectasias en NiñosCarlos Alberto QuispeAinda não há avaliações