Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Holistic Centre: Case Study 1 - Osho International Meditation Centre, Pune, IndiaDocumento4 páginasHolistic Centre: Case Study 1 - Osho International Meditation Centre, Pune, IndiaPriyesh Dubey100% (2)
- Liddell Hart PDFDocumento5 páginasLiddell Hart PDFMohamed Elkhder100% (1)
- The Wisdom BookDocumento509 páginasThe Wisdom BookRalos Latrommi100% (12)
- Petition For Bail Nonbailable LampaDocumento3 páginasPetition For Bail Nonbailable LampaNikki MendozaAinda não há avaliações
- Movie ReviewDocumento2 páginasMovie ReviewJohanna Gwenn Taganahan LomaadAinda não há avaliações
- Bank ATM Use CasesDocumento12 páginasBank ATM Use Casessbr11Ainda não há avaliações
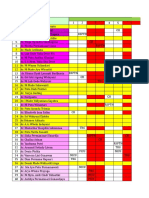
- Jadwal Rotasi Residen Ika FK Unud/Rsup Sanglah Bulan Juli 2019 SENIOR sm6,7,8Documento8 páginasJadwal Rotasi Residen Ika FK Unud/Rsup Sanglah Bulan Juli 2019 SENIOR sm6,7,8DessyadoeAinda não há avaliações
- DS Boys Weight 2-20yearsDocumento1 páginaDS Boys Weight 2-20yearsDessyadoeAinda não há avaliações
- Catatan Seputar NeuroDocumento60 páginasCatatan Seputar NeuroDessyadoeAinda não há avaliações
- Early Childhood Predictors of Anxiety in Early AdolescenceDocumento13 páginasEarly Childhood Predictors of Anxiety in Early AdolescenceDessyadoeAinda não há avaliações
- Non-Invasive High-Frequency Ventilation in Newborn Infants With Respiratory Distress (Protocol)Documento14 páginasNon-Invasive High-Frequency Ventilation in Newborn Infants With Respiratory Distress (Protocol)DessyadoeAinda não há avaliações
- 08 Ags 19Documento8 páginas08 Ags 19DessyadoeAinda não há avaliações
- 08 Ags 19Documento8 páginas08 Ags 19DessyadoeAinda não há avaliações
- Non-Invasive High-Frequency Ventilation in Newborn Infants With Respiratory Distress (Protocol)Documento14 páginasNon-Invasive High-Frequency Ventilation in Newborn Infants With Respiratory Distress (Protocol)DessyadoeAinda não há avaliações
- SKBB II Novita AssaDocumento56 páginasSKBB II Novita AssaDessyadoeAinda não há avaliações
- 325 FullDocumento20 páginas325 FullDessyadoeAinda não há avaliações
- Dr. Deasy Adoe Residen Pediatri Dr. Deasy Adoe Residen Pediatri Dr. Deasy Adoe Residen PediatriDocumento1 páginaDr. Deasy Adoe Residen Pediatri Dr. Deasy Adoe Residen Pediatri Dr. Deasy Adoe Residen PediatriDessyadoeAinda não há avaliações
- Jaga April 2019 KoreksiDocumento12 páginasJaga April 2019 KoreksiDessyadoeAinda não há avaliações
- Tyagi 2018Documento7 páginasTyagi 2018DessyadoeAinda não há avaliações
- Pneumonia Evidence-Summaries Oct-2014Documento30 páginasPneumonia Evidence-Summaries Oct-2014DessyadoeAinda não há avaliações
- NRP 2012 HandoutDocumento7 páginasNRP 2012 HandoutRina PratiwiAinda não há avaliações
- HDFCDocumento60 páginasHDFCPukhraj GehlotAinda não há avaliações
- S1-TITAN Overview BrochureDocumento8 páginasS1-TITAN Overview BrochureصصAinda não há avaliações
- SMM Live Project MICA (1) (1)Documento8 páginasSMM Live Project MICA (1) (1)Raj SinghAinda não há avaliações
- Grade 11 Stem Group 2 Practical Research 1Documento19 páginasGrade 11 Stem Group 2 Practical Research 1Roi Vincent Cuaresma BlasAinda não há avaliações
- Leadership and Turnaround Management Concepts Applied in The Agribusiness Environment in RomaniaDocumento6 páginasLeadership and Turnaround Management Concepts Applied in The Agribusiness Environment in RomaniaLoredana PredaAinda não há avaliações
- Caterpillar Cat 304.5 Mini Hydraulic Excavator (Prefix WAK) Service Repair Manual (WAK00001 and Up)Documento23 páginasCaterpillar Cat 304.5 Mini Hydraulic Excavator (Prefix WAK) Service Repair Manual (WAK00001 and Up)kfmuseddk100% (1)
- Astm A380 PDFDocumento13 páginasAstm A380 PDFaromalara12Ainda não há avaliações
- Vol. III (B) - FANSDocumento8 páginasVol. III (B) - FANSKhaled ELSaftawyAinda não há avaliações
- Muscle Building MythsDocumento5 páginasMuscle Building MythsKarolAinda não há avaliações
- B B B B: RRRR RRRRDocumento24 páginasB B B B: RRRR RRRRAnonymous TeF0kYAinda não há avaliações
- Administrative Clerk Resume TemplateDocumento2 páginasAdministrative Clerk Resume TemplateManuelAinda não há avaliações
- Flores Vs Drilon G R No 104732 June 22Documento1 páginaFlores Vs Drilon G R No 104732 June 22Henrick YsonAinda não há avaliações
- Injection Pump Test SpecificationsDocumento3 páginasInjection Pump Test Specificationsadmin tigasaudaraAinda não há avaliações
- Freedom International School Class 3 - EnglishDocumento2 páginasFreedom International School Class 3 - Englishshreyas100% (1)
- Naresh Kadyan: Voice For Animals in Rajya Sabha - Abhishek KadyanDocumento28 páginasNaresh Kadyan: Voice For Animals in Rajya Sabha - Abhishek KadyanNaresh KadyanAinda não há avaliações
- Hop Movie WorksheetDocumento3 páginasHop Movie WorksheetMARIA RIERA PRATSAinda não há avaliações
- Conflict Management and Negotiation - Team 5Documento34 páginasConflict Management and Negotiation - Team 5Austin IsaacAinda não há avaliações
- Thd04e 1Documento2 páginasThd04e 1Thao100% (1)
- On Evil - Terry EagletonDocumento44 páginasOn Evil - Terry EagletonconelcaballocansadoAinda não há avaliações
- Labor Law Highlights, 1915-2015: Labor Review Has Been in Publication. All The LegislationDocumento13 páginasLabor Law Highlights, 1915-2015: Labor Review Has Been in Publication. All The LegislationIgu jumaAinda não há avaliações
- Computer Awareness: Special Edition E-BookDocumento54 páginasComputer Awareness: Special Edition E-BookTanujit SahaAinda não há avaliações
- Use Case Diagram ShopeeDocumento6 páginasUse Case Diagram ShopeeAtmayantiAinda não há avaliações
- German Employment Visa Application: What Is A German Work Visa and Do I Need One?Documento4 páginasGerman Employment Visa Application: What Is A German Work Visa and Do I Need One?FarbodAinda não há avaliações
- B. Complete The Following Exercise With or Forms of The Indicated VerbsDocumento4 páginasB. Complete The Following Exercise With or Forms of The Indicated VerbsLelyLealGonzalezAinda não há avaliações