Você também pode gostar
- Government College of Nursing: Procedure ONDocumento6 páginasGovernment College of Nursing: Procedure ONpriyanka100% (5)
- Skeletal Plan ON Embryological and Fetal Development: Submitted To: Submitted byDocumento11 páginasSkeletal Plan ON Embryological and Fetal Development: Submitted To: Submitted byPabhat Kumar100% (1)
- Introduction - :: 1. Pre Embryonic PeriodDocumento11 páginasIntroduction - :: 1. Pre Embryonic PeriodPabhat Kumar100% (1)
- First Stage of LabourDocumento14 páginasFirst Stage of LabourAnuradha Maurya100% (3)
- Case Study On PROMDocumento11 páginasCase Study On PROMPabhat Kumar86% (7)
- Multiple Pregnancy: Presented byDocumento49 páginasMultiple Pregnancy: Presented byvarshasharma05Ainda não há avaliações
- Problems With Passenger and PowerDocumento6 páginasProblems With Passenger and PowerhoohooAinda não há avaliações
- Nursing StandardsDocumento16 páginasNursing StandardsPabhat KumarAinda não há avaliações
- OB MustKnowsDocumento90 páginasOB MustKnowsHarlyn MagsinoAinda não há avaliações
- Cervical DystociaDocumento22 páginasCervical DystociaBaldau TiwariAinda não há avaliações
- Genital Tract InjuriesDocumento24 páginasGenital Tract InjuriesManisha ThakurAinda não há avaliações
- Induction of LabourDocumento18 páginasInduction of LabourNihal ZaidiAinda não há avaliações
- Manual Removal of PlacentaDocumento2 páginasManual Removal of PlacentaKrishnaveni Murugesh100% (1)
- Uterine MalformationsDocumento6 páginasUterine MalformationssubashikAinda não há avaliações
- ObGyn Outline BeckmannDocumento85 páginasObGyn Outline Beckmannp4sierra50% (2)
- Gynacology and Obstetrics Format For History & Physical ExaminaitonDocumento13 páginasGynacology and Obstetrics Format For History & Physical ExaminaitonBayisa GirmaAinda não há avaliações
- Procedure On Vaginal ExaminationDocumento7 páginasProcedure On Vaginal ExaminationPriya100% (2)
- Labor and DeliveryDocumento50 páginasLabor and DeliveryAce Cabilan100% (1)
- 3rd Stage of LabourDocumento10 páginas3rd Stage of LabourBhawna JoshiAinda não há avaliações
- Elderly PrimiDocumento7 páginasElderly PrimiAnnapurna Dangeti67% (3)
- The Average Blood Loss Following Vaginal Delivery, Cesarean Delivery and Cesarean Hysterectomy Is 500 ML, 1000 ML and 1500 ML RespectivelyDocumento11 páginasThe Average Blood Loss Following Vaginal Delivery, Cesarean Delivery and Cesarean Hysterectomy Is 500 ML, 1000 ML and 1500 ML RespectivelypriyankaAinda não há avaliações
- Antenatal Care & ManagementDocumento22 páginasAntenatal Care & ManagementPabhat Kumar100% (3)
- Case Presentation On PROM EDITedDocumento15 páginasCase Presentation On PROM EDITedPabhat Kumar40% (5)
- Management of Cardiac Disease in PregnancyDocumento7 páginasManagement of Cardiac Disease in PregnancyMegavarnen Gobinathan100% (1)
- Seminar On Complication of 3rd Stage PPHDocumento13 páginasSeminar On Complication of 3rd Stage PPHjuhi labana0% (1)
- Procedure Manual For Obstetrics and Gynecological Nursing: Government College of Nursing Somajiguda, Hyderabad, T.SDocumento119 páginasProcedure Manual For Obstetrics and Gynecological Nursing: Government College of Nursing Somajiguda, Hyderabad, T.SBlessy Madhuri100% (5)
- Management of LabourDocumento16 páginasManagement of LabourAlbert MusinguziAinda não há avaliações
- Parse TheoryDocumento33 páginasParse TheoryPabhat Kumar100% (2)
- PARTOGRAPHDocumento9 páginasPARTOGRAPHطاہر محمودAinda não há avaliações
- Antenatal CareDocumento19 páginasAntenatal CareIshika RoyAinda não há avaliações
- Abortion PP TDocumento42 páginasAbortion PP TDivya ToppoAinda não há avaliações
- Antenatal Care & ManagementDocumento23 páginasAntenatal Care & ManagementPabhat Kumar100% (1)
- Antenatal Care & ManagementDocumento23 páginasAntenatal Care & ManagementPabhat Kumar100% (1)
- Prolong LabourDocumento5 páginasProlong LabourNishaThakuri100% (1)
- Diagnostic Modalities in PregnancyDocumento11 páginasDiagnostic Modalities in PregnancyRavina Patel100% (1)
- Physiology of LabourDocumento40 páginasPhysiology of LabourShubhi VaivhareAinda não há avaliações
- Insertion of Iucd AssessmentDocumento6 páginasInsertion of Iucd AssessmentKaku ManishaAinda não há avaliações
- Seminar On Abnormal Labour and Its ManagementDocumento40 páginasSeminar On Abnormal Labour and Its ManagementMonika Bagchi100% (4)
- National College of Nursing: Procedure ONDocumento6 páginasNational College of Nursing: Procedure ONSumit Yadav100% (1)
- PartographDocumento33 páginasPartographKathrynne Mendoza100% (1)
- Antenatal CareDocumento3 páginasAntenatal CareAnnapurna DangetiAinda não há avaliações
- Mechanism of LabourDocumento18 páginasMechanism of LabournamithaAinda não há avaliações
- Minor Disorders of Newborn and Its ManagementDocumento3 páginasMinor Disorders of Newborn and Its Managementarun26198891% (11)
- Injuries To The Birth CanalDocumento67 páginasInjuries To The Birth CanalnamitaAinda não há avaliações
- Procedure ON: Copper-T InsertionDocumento5 páginasProcedure ON: Copper-T Insertionpriyanka100% (2)
- Case Presentation On Pre-EclampsiaDocumento18 páginasCase Presentation On Pre-EclampsiaPabhat Kumar86% (7)
- AntenatalDocumento5 páginasAntenatalPabhat KumarAinda não há avaliações
- AntenatalDocumento5 páginasAntenatalPabhat KumarAinda não há avaliações
- Case Study On Normal Vaginal DeliveryDocumento24 páginasCase Study On Normal Vaginal DeliveryPabhat Kumar80% (30)
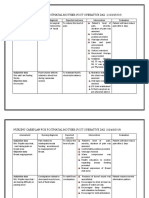
- Nursing Care Plan Assessment Nursing Diagnosis Nursing Goal Nursing Intervention Rationale Outcome Criteria Actual EvaluationDocumento4 páginasNursing Care Plan Assessment Nursing Diagnosis Nursing Goal Nursing Intervention Rationale Outcome Criteria Actual EvaluationPabhat Kumar50% (2)
- Normal Labor Essential Factors Elements of Uterine Contractions & Physiology of 1 Stage of LaborDocumento88 páginasNormal Labor Essential Factors Elements of Uterine Contractions & Physiology of 1 Stage of LaborAswathy Aswathy100% (1)
- Obg - AntentalDocumento57 páginasObg - AntentalA suhasini0% (1)
- Antenatal AssessmentDocumento67 páginasAntenatal Assessmenthiral mistry100% (2)
- Lesson Plan of Lab Demo Face PresentationDocumento17 páginasLesson Plan of Lab Demo Face PresentationShalu Bohra Manola100% (1)
- DEMONSTRATION On Care of BreastDocumento12 páginasDEMONSTRATION On Care of BreastRaja100% (3)
- Power Passages and Passenger PDFDocumento13 páginasPower Passages and Passenger PDFNestley TiongsonAinda não há avaliações
- Managament of The 2nd Stage of LabourDocumento53 páginasManagament of The 2nd Stage of LabourJSeashark100% (1)
- Physiology and Management of 1St Stage of LabourDocumento5 páginasPhysiology and Management of 1St Stage of LabourSucharita PandaAinda não há avaliações
- Abnormal Uterine ActionDocumento27 páginasAbnormal Uterine Actiontanmai noolu100% (1)
- Planned ParenthoodDocumento34 páginasPlanned Parenthoodvincentsharon80% (5)
- Newborn Assessment OBGDocumento6 páginasNewborn Assessment OBGAnish VeettiyankalAinda não há avaliações
- Case Presentation On PROM New...... EDITDocumento18 páginasCase Presentation On PROM New...... EDITPabhat Kumar100% (2)
- Antenatal Care & Management NewDocumento23 páginasAntenatal Care & Management NewPabhat Kumar100% (4)
- Antenatal Care & Management NewDocumento23 páginasAntenatal Care & Management NewPabhat Kumar100% (4)
- Antenatal Assessment of Foetal Wellbeing.Documento30 páginasAntenatal Assessment of Foetal Wellbeing.Kavya S MohanAinda não há avaliações
- Obstetrics and GynecologyDocumento408 páginasObstetrics and GynecologyNurseNancy93100% (5)
- PPTCT Policy Guideline PDFDocumento31 páginasPPTCT Policy Guideline PDFPabhat KumarAinda não há avaliações
- PPTCT Policy Guideline PDFDocumento31 páginasPPTCT Policy Guideline PDFPabhat KumarAinda não há avaliações
- Procedure On Techniques of BreastfeedingDocumento5 páginasProcedure On Techniques of BreastfeedingPabhat Kumar100% (2)
- Gynecological ProceduresDocumento17 páginasGynecological Proceduresjeelani saima100% (5)
- Antenatal ExaminationDocumento18 páginasAntenatal ExaminationAnonymous ExR0zw100% (2)
- Antenatal ExaminationDocumento18 páginasAntenatal ExaminationAnonymous 0C4OZmR100% (1)
- Maternal, Morbidity, Mortality and Fertility RatesDocumento18 páginasMaternal, Morbidity, Mortality and Fertility Ratesmadhu.BAinda não há avaliações
- Lesson Plan On Operative DeliveryDocumento13 páginasLesson Plan On Operative DeliveryArjun NeupaneAinda não há avaliações
- Case Study..Care PlanDocumento6 páginasCase Study..Care PlanPabhat Kumar0% (1)
- Case Study..Care PlanDocumento6 páginasCase Study..Care PlanPabhat Kumar0% (1)
- LESSON PLAN On Legal & Ethical IssueDocumento4 páginasLESSON PLAN On Legal & Ethical IssuePabhat Kumar80% (5)
- Cephalo Pelvic DisproportionDocumento43 páginasCephalo Pelvic DisproportionPabhat KumarAinda não há avaliações
- Antenatal AssessmentDocumento16 páginasAntenatal AssessmentDevuchandana RAinda não há avaliações
- Antenatal Care PPT EchyDocumento14 páginasAntenatal Care PPT EchyYuliana alensi falloAinda não há avaliações
- Antenatal ExaminationDocumento2 páginasAntenatal ExaminationJunaidahMubarakAliAinda não há avaliações
- Demo AntenatalDocumento26 páginasDemo AntenatalDeepika PatidarAinda não há avaliações
- Postpartum Hemorrhage (PPH) : Prakash Thakulla InternDocumento38 páginasPostpartum Hemorrhage (PPH) : Prakash Thakulla InternPrakash ThakullaAinda não há avaliações
- Procedure Assignment For ManagementDocumento7 páginasProcedure Assignment For ManagementPatel Amee100% (1)
- Genital Tract InjuriesDocumento19 páginasGenital Tract InjuriesMarvella Nongkhar100% (1)
- Copper T InsertionDocumento19 páginasCopper T Insertionapi-3823785100% (2)
- Government College of Nursing Jodhpur: Procedure On-Cordocentesis Subject-Obstetrics & Gynecology Specialty-IDocumento4 páginasGovernment College of Nursing Jodhpur: Procedure On-Cordocentesis Subject-Obstetrics & Gynecology Specialty-Ipriyanka100% (2)
- Ob Seminar Amniotic Fluid-1Documento25 páginasOb Seminar Amniotic Fluid-1Aleena Davis100% (1)
- Cord Presentation and ProlapseDocumento4 páginasCord Presentation and ProlapseAnnapurna Dangeti100% (2)
- Abnormal LaborDocumento20 páginasAbnormal Laborأ.م.د. إنعام فيصل محمدAinda não há avaliações
- HydramniosDocumento31 páginasHydramniosSpandana DepuruAinda não há avaliações
- (11-13) Assess The Knowledge On Minor Ailments of Pregnancy-FormatDocumento3 páginas(11-13) Assess The Knowledge On Minor Ailments of Pregnancy-FormatMudasir Ahmad BhatAinda não há avaliações
- KMCPPT 170927065907 PDFDocumento30 páginasKMCPPT 170927065907 PDFPabhat KumarAinda não há avaliações
- TataNeuApp 1MG 1701053400200Documento1 páginaTataNeuApp 1MG 1701053400200Pabhat KumarAinda não há avaliações
- Surgical MenopauseDocumento12 páginasSurgical MenopausePabhat Kumar100% (1)
- Maxims Hand Out 2Documento1 páginaMaxims Hand Out 2Pabhat KumarAinda não há avaliações
- Questionnaire: Questionarrie Part-A Code NumberDocumento5 páginasQuestionnaire: Questionarrie Part-A Code NumberPabhat KumarAinda não há avaliações
- A Report On Attending A ConferenceDocumento5 páginasA Report On Attending A ConferencePabhat KumarAinda não há avaliações
- Skeletal Plan ON National Health Program Related To Child HealthDocumento3 páginasSkeletal Plan ON National Health Program Related To Child HealthPabhat KumarAinda não há avaliações
- Bibliography Content M.L.aDocumento13 páginasBibliography Content M.L.aPabhat KumarAinda não há avaliações
- ABSTRACT ItismitaDocumento4 páginasABSTRACT ItismitaPabhat KumarAinda não há avaliações
- Malposition - Malpresentation (L)Documento35 páginasMalposition - Malpresentation (L)Touseef Ur RehmanAinda não há avaliações
- Intrapartal CareDocumento14 páginasIntrapartal CareCheryl OrtizAinda não há avaliações
- Handout # 10Documento22 páginasHandout # 10Ram August100% (1)
- Fetal Malpresentation and Malposition - LecturioDocumento17 páginasFetal Malpresentation and Malposition - LecturiomeddcrossAinda não há avaliações
- PrematurityDocumento37 páginasPrematurityNishaThakuriAinda não há avaliações
- 1 Labor and Delivery ProcessDocumento13 páginas1 Labor and Delivery ProcessBardiaga JmayAinda não há avaliações
- Intrapartum (Process of Labor Delivery)Documento206 páginasIntrapartum (Process of Labor Delivery)coosa liquorsAinda não há avaliações
- Case 1Documento9 páginasCase 1Saketha Rama ReddyAinda não há avaliações
- Topic - 5Documento96 páginasTopic - 5Sub 7 Grp 3Ainda não há avaliações
- 3Documento6 páginas3Yuuki Chitose (tai-kun)Ainda não há avaliações
- Maternal Assessment: History TakingDocumento18 páginasMaternal Assessment: History TakingSirisha ChelvaAinda não há avaliações
- Labor and Birth NotesDocumento36 páginasLabor and Birth NotesJodi BairAinda não há avaliações
- Familymedicine 3 1086 PDFDocumento8 páginasFamilymedicine 3 1086 PDFApryana Damayanti ARAinda não há avaliações
- Duty Report 5.12.1978Documento55 páginasDuty Report 5.12.1978Riyan W. PratamaAinda não há avaliações
- Script Leopold Maneuver & Fundal HeightDocumento5 páginasScript Leopold Maneuver & Fundal HeightUNA YVONNE DOMANTAYAinda não há avaliações
- LaborDocumento69 páginasLaborzamurd76Ainda não há avaliações
- Ok Hi RekapDocumento48 páginasOk Hi RekapRafika Novianti CikovaAinda não há avaliações
- PATHO OB DystociaDocumento14 páginasPATHO OB Dystociasailor MoonAinda não há avaliações
- CR Duty 09.05.2019Documento87 páginasCR Duty 09.05.2019R Ismail HadyathmaAinda não há avaliações