Você também pode gostar
- HKDSE English 2020: Tips for Expository Essays and ReportsDocumento94 páginasHKDSE English 2020: Tips for Expository Essays and ReportsLeroy Cheng100% (1)
- Event 201 Transcript Explores Global Pandemic PreparednessDocumento54 páginasEvent 201 Transcript Explores Global Pandemic Preparednessyisole100% (2)
- Near Death ExperienceDocumento10 páginasNear Death ExperienceAARYENDRA100% (1)
- Complementary and Alternative Medical Lab Testing Part 8: UrologyNo EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyNota: 3 de 5 estrelas3/5 (1)
- Hi Yield Goljan Pathology Review MemorizeDocumento57 páginasHi Yield Goljan Pathology Review MemorizeTrisAinda não há avaliações
- Delayed Cord Clamping Reduces Mortality in Preterm InfantsDocumento37 páginasDelayed Cord Clamping Reduces Mortality in Preterm InfantsAndi DeviriyantiAinda não há avaliações
- ASA Physical Status ClassificationDocumento1 páginaASA Physical Status ClassificationАндрій ДанильцівAinda não há avaliações
- Chapter 2 Overcoming MS Handbook - SamplerDocumento20 páginasChapter 2 Overcoming MS Handbook - SamplerAllen & UnwinAinda não há avaliações
- SJK(T) Ladang Seremban Final ExamDocumento9 páginasSJK(T) Ladang Seremban Final ExamUganes WariAinda não há avaliações
- Sindhu Final ThesisDocumento122 páginasSindhu Final Thesiskrishnasree100% (2)
- Polymorphisms of Interleukin-10 Promoter Are Not Associated With Prognosis of Advanced Gastric CancerDocumento6 páginasPolymorphisms of Interleukin-10 Promoter Are Not Associated With Prognosis of Advanced Gastric CancerMona MostafaAinda não há avaliações
- PVC ArticleDocumento7 páginasPVC ArticleSergio Mauricio Segura ArenasAinda não há avaliações
- Effects of Acute Critical Illnesses On The Performance of Interferongamma Release AssayDocumento9 páginasEffects of Acute Critical Illnesses On The Performance of Interferongamma Release Assayt45tz5hfsfAinda não há avaliações
- Incidence and Risk Factors of Anti-Tuberculosis DRDocumento11 páginasIncidence and Risk Factors of Anti-Tuberculosis DRDi LaAinda não há avaliações
- Association Between Polymorphisms in CXCR2 Gene and PreeclampsiaDocumento8 páginasAssociation Between Polymorphisms in CXCR2 Gene and PreeclampsiaalyneAinda não há avaliações
- 11 - Manoj Kumar MinjDocumento8 páginas11 - Manoj Kumar MinjIndah SarihandayaniAinda não há avaliações
- Pregnancy HypertensionDocumento7 páginasPregnancy HypertensionEgi NabilaAinda não há avaliações
- Evaluation of Serum Lipids in Preeclampsia: A Comparative StudyDocumento4 páginasEvaluation of Serum Lipids in Preeclampsia: A Comparative StudyGladys SusantyAinda não há avaliações
- International Journal of Gynecology and ObstetricsDocumento5 páginasInternational Journal of Gynecology and ObstetricsWilliams Alejandro Choroco VillegasAinda não há avaliações
- Office-Based Point of Care Testing (Iga/Igg-Deamidated Gliadin Peptide) For Celiac DiseaseDocumento9 páginasOffice-Based Point of Care Testing (Iga/Igg-Deamidated Gliadin Peptide) For Celiac DiseasemarcosAinda não há avaliações
- Pre and Post Conception Risk Factors in PROM: Research ArticleDocumento5 páginasPre and Post Conception Risk Factors in PROM: Research ArticleNurul ImaniarAinda não há avaliações
- Thyroid Abnormalities in Paediatric Patients With Vitiligo: Retrospective StudyDocumento3 páginasThyroid Abnormalities in Paediatric Patients With Vitiligo: Retrospective StudySarah Humaira DennisonAinda não há avaliações
- PCT biomarker accurately diagnoses pediatric appendicitisDocumento6 páginasPCT biomarker accurately diagnoses pediatric appendicitisGilang IrwansyahAinda não há avaliações
- Diagnostics 11 01659Documento7 páginasDiagnostics 11 01659Roni wahyu hidayatiAinda não há avaliações
- Effects of Chronic Lymphocytic Thyroiditis On The Clinicopathological Features of Papillary Thyroid CancerDocumento7 páginasEffects of Chronic Lymphocytic Thyroiditis On The Clinicopathological Features of Papillary Thyroid CancerRahmawati RdnAinda não há avaliações
- Acute Pyelonephritis in PregnancyDocumento7 páginasAcute Pyelonephritis in PregnancyKvmLlyAinda não há avaliações
- Ijsred V2i1p1Documento6 páginasIjsred V2i1p1IJSREDAinda não há avaliações
- Epi y CancerDocumento6 páginasEpi y CancerKatherin PeñafielAinda não há avaliações
- BJC 2017154Documento8 páginasBJC 2017154Altair CamargoAinda não há avaliações
- Office-Based Point of Care Testing (Iga/Igg-Deamidated Gliadin Peptide) For Celiac DiseaseDocumento10 páginasOffice-Based Point of Care Testing (Iga/Igg-Deamidated Gliadin Peptide) For Celiac DiseaseGrecia BocuAinda não há avaliações
- Case-Finding in Primary Care For Coeliac Disease: Accuracy and Cost-Effectiveness of A Rapid Point-Of-Care TestDocumento11 páginasCase-Finding in Primary Care For Coeliac Disease: Accuracy and Cost-Effectiveness of A Rapid Point-Of-Care TestmarcosAinda não há avaliações
- CC 12918Documento59 páginasCC 12918Romica MarcanAinda não há avaliações
- Journal of SGPTDocumento3 páginasJournal of SGPTEric GibsonAinda não há avaliações
- Deng 2012Documento4 páginasDeng 2012Rachmad RasidinAinda não há avaliações
- Simtomax: A New Screening Tool For Coeliac Disease: Linda MizenDocumento6 páginasSimtomax: A New Screening Tool For Coeliac Disease: Linda MizenmarcosAinda não há avaliações
- FullPIERS Paper-LancetDocumento39 páginasFullPIERS Paper-LancetRyan SadonoAinda não há avaliações
- Tenofovir Associated Renal Toxicity in A Cohort of Hiv Infected Individuals in Goa - January - 2020 - 1577784624 - 0401138Documento3 páginasTenofovir Associated Renal Toxicity in A Cohort of Hiv Infected Individuals in Goa - January - 2020 - 1577784624 - 0401138rfrdefAinda não há avaliações
- Nihms 82233Documento10 páginasNihms 82233LeonardoAinda não há avaliações
- Clinical Significance of UGT1A1 GeneticDocumento8 páginasClinical Significance of UGT1A1 GeneticAsri RachmawatiAinda não há avaliações
- Leucocyte Differential Count May Predict Risk of Pregnancy Induced HypertensionDocumento10 páginasLeucocyte Differential Count May Predict Risk of Pregnancy Induced Hypertensionhypebeast dopeAinda não há avaliações
- Neutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisDocumento7 páginasNeutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisHamza AhmedAinda não há avaliações
- tmpC1E4 TMPDocumento6 páginastmpC1E4 TMPFrontiersAinda não há avaliações
- Sindrom NefrotikDocumento7 páginasSindrom NefrotikDania SaraswatiAinda não há avaliações
- ArticleDocumento16 páginasArticleobbyAinda não há avaliações
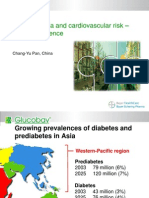
- Asia - Pan - Dysglycaemia and Cardiovascular Risk Û Asian ExperienceDocumento18 páginasAsia - Pan - Dysglycaemia and Cardiovascular Risk Û Asian ExperienceputrakartonoAinda não há avaliações
- Hellp 2Documento7 páginasHellp 2Nur Rahmat WibowoAinda não há avaliações
- Multifetal PregnanciesDocumento32 páginasMultifetal PregnanciesSheilla KhonadaAinda não há avaliações
- 5 - Diabetes MellitusDocumento9 páginas5 - Diabetes MellitusNatnicha foongfaAinda não há avaliações
- Dengue Fever During Pregnancy: Original PaperDocumento7 páginasDengue Fever During Pregnancy: Original Papermuhammad alfarisi sutrisnoAinda não há avaliações
- 10 1016@j Jhep 2020 10 009Documento6 páginas10 1016@j Jhep 2020 10 009Adelina HorhatAinda não há avaliações
- Original Article: Clinical and Laboratory Features of Typhoid Fever in ChildhoodDocumento6 páginasOriginal Article: Clinical and Laboratory Features of Typhoid Fever in ChildhoodRidha Surya NugrahaAinda não há avaliações
- Feig 2017Documento13 páginasFeig 2017Lembaga Pendidikan dan PelayananAinda não há avaliações
- Chakra - Factors Associated With Complications of C DiffDocumento8 páginasChakra - Factors Associated With Complications of C DiffCherry SmileAinda não há avaliações
- IJCRT23A5059Documento9 páginasIJCRT23A5059Agus SunardiAinda não há avaliações
- Prolonged Latency of Preterm Premature Rupture of Membranes and Risk of Neonatal SepsisDocumento6 páginasProlonged Latency of Preterm Premature Rupture of Membranes and Risk of Neonatal SepsisYudhi AuliaAinda não há avaliações
- Weekly Task at Pediatric Intensive Unite (Picu) 1Documento9 páginasWeekly Task at Pediatric Intensive Unite (Picu) 1Reem ApadiAinda não há avaliações
- Interleukin-10 and Interferon Gamma Gene Polymorphisms and Hepatitis C Virus-Related Liver Cirrhosis RiskDocumento6 páginasInterleukin-10 and Interferon Gamma Gene Polymorphisms and Hepatitis C Virus-Related Liver Cirrhosis RiskdedeshyfaAinda não há avaliações
- ERC 15 0145.fullDocumento31 páginasERC 15 0145.fullAdityaGedeAinda não há avaliações
- 2 Dümichen2012Documento6 páginas2 Dümichen2012Sergio SampaioAinda não há avaliações
- Robin P. Trombosis ResearchDocumento6 páginasRobin P. Trombosis Researchabarquet3101Ainda não há avaliações
- Maternal Outcome in Relation To Biochemical Parameters in Hypertensive Disorders in PregnancyDocumento5 páginasMaternal Outcome in Relation To Biochemical Parameters in Hypertensive Disorders in PregnancyHendrikusAinda não há avaliações
- GO Niveles Circulantes de CA135 en Mujeres PerimenopáusicasDocumento11 páginasGO Niveles Circulantes de CA135 en Mujeres PerimenopáusicasC T AAinda não há avaliações
- Zinc Transporter 8 Autoantibody in The Diagnosis of Type 1 Diabetes in ChildrenDocumento11 páginasZinc Transporter 8 Autoantibody in The Diagnosis of Type 1 Diabetes in ChildrenEva EphoelAinda não há avaliações
- Prevalence of ZnT8 Antibody in Turkish Children and AdolescentsDocumento5 páginasPrevalence of ZnT8 Antibody in Turkish Children and AdolescentsFairuza NafilahAinda não há avaliações
- 1307-Article Text-3852-1-10-20170616Documento6 páginas1307-Article Text-3852-1-10-20170616Dalila BackupAinda não há avaliações
- Early Acute Kidney Injury Predicts Progressive Renal Dysfunction and Higher Mortality in Severely Burned AdultsDocumento23 páginasEarly Acute Kidney Injury Predicts Progressive Renal Dysfunction and Higher Mortality in Severely Burned AdultsKartika JuwitaAinda não há avaliações
- Hum. Reprod.-2004-Carp-191-5Documento5 páginasHum. Reprod.-2004-Carp-191-5venkayammaAinda não há avaliações
- Leptin rs2167270 G A (G19A) Polymorphism May Decrease The Risk of Cancer: A Case Control Study and Meta Analysis Involving 19 989 SubjectsDocumento10 páginasLeptin rs2167270 G A (G19A) Polymorphism May Decrease The Risk of Cancer: A Case Control Study and Meta Analysis Involving 19 989 SubjectsAlfa FebriandaAinda não há avaliações
- Higado Graso Agudo en El Embarazo AJG 2017Documento9 páginasHigado Graso Agudo en El Embarazo AJG 2017Fabrizzio BardalesAinda não há avaliações
- AflpDocumento8 páginasAflprmiguel7Ainda não há avaliações
- Differences in Sexual Function After Vaginal DeliveryDocumento3 páginasDifferences in Sexual Function After Vaginal DeliveryAlfa FebriandaAinda não há avaliações
- Poster Session IV: ObjectiveDocumento2 páginasPoster Session IV: ObjectiveAlfa FebriandaAinda não há avaliações
- CMJ 57 6 Peterlin 28051281Documento6 páginasCMJ 57 6 Peterlin 28051281Alfa FebriandaAinda não há avaliações
- Corticotrophin Releasing Hormone As A Useful Marker To Identify The Pre-EclampsiaDocumento4 páginasCorticotrophin Releasing Hormone As A Useful Marker To Identify The Pre-EclampsiaAlfa FebriandaAinda não há avaliações
- Magnesium OyeDocumento11 páginasMagnesium Oyeade_fkuAinda não há avaliações
- Aavs 7 1 17-23 PDFDocumento7 páginasAavs 7 1 17-23 PDFAlfa FebriandaAinda não há avaliações
- Haplotype AnalysisDocumento5 páginasHaplotype AnalysisAlfa FebriandaAinda não há avaliações
- Haplotype AnalysisDocumento5 páginasHaplotype AnalysisAlfa FebriandaAinda não há avaliações
- Pregnancy and Postpartum Risks for Venous ThrombosisDocumento6 páginasPregnancy and Postpartum Risks for Venous ThrombosisAlfa FebriandaAinda não há avaliações
- Prothrombin and Factor V Mutations in Women With ADocumento7 páginasProthrombin and Factor V Mutations in Women With AAlfa FebriandaAinda não há avaliações
- Pregnancy and Postpartum Risks for Venous ThrombosisDocumento6 páginasPregnancy and Postpartum Risks for Venous ThrombosisAlfa FebriandaAinda não há avaliações
- Antenatal Care of Preeclampsia: From The Inverted Pyramid To The Arrow Model?Documento4 páginasAntenatal Care of Preeclampsia: From The Inverted Pyramid To The Arrow Model?Alfa FebriandaAinda não há avaliações
- Antenatal Care of Preeclampsia: From The Inverted Pyramid To The Arrow Model?Documento4 páginasAntenatal Care of Preeclampsia: From The Inverted Pyramid To The Arrow Model?Alfa FebriandaAinda não há avaliações
- CMJ 57 6 Peterlin 28051281Documento6 páginasCMJ 57 6 Peterlin 28051281Alfa FebriandaAinda não há avaliações
- A Rare Case of Meigs Syndrome in Pregnancy With Bilateral Ovarian MassesDocumento2 páginasA Rare Case of Meigs Syndrome in Pregnancy With Bilateral Ovarian MassesAlfa FebriandaAinda não há avaliações
- Single Nucleotide Polymorphisms of Follicle-Stimulating Hormone Receptor Promoter and Their Impacts To The Promoter ActivitiesDocumento10 páginasSingle Nucleotide Polymorphisms of Follicle-Stimulating Hormone Receptor Promoter and Their Impacts To The Promoter ActivitiesAlfa FebriandaAinda não há avaliações
- Aogs 13082Documento8 páginasAogs 13082Alfa FebriandaAinda não há avaliações
- TRF 12966Documento8 páginasTRF 12966Alfa FebriandaAinda não há avaliações
- JokohjokDocumento2 páginasJokohjokAlfa FebriandaAinda não há avaliações
- Success of External Cephalic Version With Terbutaline As Tocolytic AgentDocumento4 páginasSuccess of External Cephalic Version With Terbutaline As Tocolytic AgentAlfa FebriandaAinda não há avaliações
- Endometriosis-Associated Infertility Causes and TreatmentsDocumento9 páginasEndometriosis-Associated Infertility Causes and TreatmentsAlfa FebriandaAinda não há avaliações
- Meigs' Syndrome and Pseudo-Meigs' Syndrome: Report of Four Cases and Literature ReviewsDocumento6 páginasMeigs' Syndrome and Pseudo-Meigs' Syndrome: Report of Four Cases and Literature ReviewsAlfa FebriandaAinda não há avaliações
- 1 PDFDocumento7 páginas1 PDFAlfa FebriandaAinda não há avaliações
- Iron Deficiency Anaemia In...Documento9 páginasIron Deficiency Anaemia In...Alfa FebriandaAinda não há avaliações
- Anaemia Pregnancy: (Dieckmann 1944 I960)Documento13 páginasAnaemia Pregnancy: (Dieckmann 1944 I960)Alfa FebriandaAinda não há avaliações
- Transfusion-Related Acute Lung Injury Risk Mitigation: An UpdateDocumento10 páginasTransfusion-Related Acute Lung Injury Risk Mitigation: An UpdateAlfa FebriandaAinda não há avaliações
- Brian Chang CV - 2020Documento8 páginasBrian Chang CV - 2020Brian ChangAinda não há avaliações
- Ilovepdf MergedDocumento45 páginasIlovepdf Mergedacte minophenAinda não há avaliações
- Material Identification: Recommended Use and Use RestrictionDocumento7 páginasMaterial Identification: Recommended Use and Use RestrictionPROYECTOS CIMIAinda não há avaliações
- Health WorkersDocumento19 páginasHealth WorkersAmna HayatAinda não há avaliações
- Internal Medicine #1Documento167 páginasInternal Medicine #1Nikhil RayarakulaAinda não há avaliações
- Star Health Assure - One Pager - Version 1.0 - April - 2022Documento3 páginasStar Health Assure - One Pager - Version 1.0 - April - 2022Shihb100% (1)
- Hearing Status of Children Under Five Years Old in Jatinangor DistrictDocumento5 páginasHearing Status of Children Under Five Years Old in Jatinangor DistricterickAinda não há avaliações
- Prosiding ICHR - Perceived Barriers Related To School MentalDocumento11 páginasProsiding ICHR - Perceived Barriers Related To School MentalRofingatul MubasyirohAinda não há avaliações
- The Aids Myth: Karl Horst PoehlmannDocumento5 páginasThe Aids Myth: Karl Horst Poehlmanncolompar80Ainda não há avaliações
- 12 - Terapia Pulpar para Dientes Primarios y Permanentes JovenesDocumento4 páginas12 - Terapia Pulpar para Dientes Primarios y Permanentes JovenesJeanAinda não há avaliações
- Psychosomatic Pain: Ertuğrul AllahverdiDocumento20 páginasPsychosomatic Pain: Ertuğrul AllahverdidiasAinda não há avaliações
- Debre Markos University Epidemiology ScreeningDocumento55 páginasDebre Markos University Epidemiology ScreeningTewodros AntenehAinda não há avaliações
- HISTORY OF MEDICINEDocumento2 páginasHISTORY OF MEDICINEMonsour SalazarAinda não há avaliações
- Central Academy: General InstructionsDocumento7 páginasCentral Academy: General InstructionsShyam SoniAinda não há avaliações
- A List of Highly in Uential Biomedical Researchers Until2011Documento27 páginasA List of Highly in Uential Biomedical Researchers Until2011Hua Hidari YangAinda não há avaliações
- Krizelle CAPP 2Documento2 páginasKrizelle CAPP 2Krizelle VaronaAinda não há avaliações
- Myhealth Suraksha-Policy WordingDocumento39 páginasMyhealth Suraksha-Policy Wordingjio325113Ainda não há avaliações
- Neural ApoptosisDocumento6 páginasNeural ApoptosisJay HardkickAinda não há avaliações
- Teledentistry Solutions for Dentistry During COVID-19Documento7 páginasTeledentistry Solutions for Dentistry During COVID-19Dio Nella ArlinggaAinda não há avaliações
- MSN QUESTION BANK- POST OPERATIVE MANAGEMENT OF MASTOIDITISDocumento31 páginasMSN QUESTION BANK- POST OPERATIVE MANAGEMENT OF MASTOIDITISkiran kumarAinda não há avaliações
- Iron Deficiency AnemiaDocumento16 páginasIron Deficiency AnemiaSaboorMalikAinda não há avaliações
- Goal/s: After 20 Minutes of Nurse-Client Interaction, Client Will Be Knowledgeable About Newly Diagnosed Condition (Acute Appendicitis)Documento3 páginasGoal/s: After 20 Minutes of Nurse-Client Interaction, Client Will Be Knowledgeable About Newly Diagnosed Condition (Acute Appendicitis)Rhn pjtAinda não há avaliações