Você também pode gostar
- USIR NCYP Therapeutic Rel FINALGF26novDocumento13 páginasUSIR NCYP Therapeutic Rel FINALGF26novhimmatul aliyahAinda não há avaliações
- Nursing Theories and Practice Smith Marlaine C SRG PDFDocumento565 páginasNursing Theories and Practice Smith Marlaine C SRG PDFLerma Delasondra100% (1)
- Coursebook-English For Nurses PDFDocumento49 páginasCoursebook-English For Nurses PDFhimmatul aliyahAinda não há avaliações
- Coursebook-English For Nurses PDFDocumento49 páginasCoursebook-English For Nurses PDFhimmatul aliyah100% (1)
- Establishing Therapeutic Relationships PDFDocumento62 páginasEstablishing Therapeutic Relationships PDFChander KantaAinda não há avaliações
- Normal Bone Anatomy and PhysiologyDocumento9 páginasNormal Bone Anatomy and PhysiologyElsa GonçalvesAinda não há avaliações
- SMG Clinical Best Practices Print BW NauseaDocumento25 páginasSMG Clinical Best Practices Print BW Nauseahimmatul aliyahAinda não há avaliações
- Establishing Therapeutic Relationships PDFDocumento62 páginasEstablishing Therapeutic Relationships PDFChander KantaAinda não há avaliações
- SMG Clinical Best Practices Print BW NauseaDocumento25 páginasSMG Clinical Best Practices Print BW Nauseahimmatul aliyahAinda não há avaliações
- Early Diagnosis of Acute Myocardial Infarction Using High-Sensitivity Troponin IDocumento10 páginasEarly Diagnosis of Acute Myocardial Infarction Using High-Sensitivity Troponin Ihimmatul aliyahAinda não há avaliações
- Nursing TeoriDocumento4 páginasNursing Teorihimmatul aliyahAinda não há avaliações
- GastritisDocumento9 páginasGastritishimmatul aliyahAinda não há avaliações
- Jurnal Turner PDFDocumento13 páginasJurnal Turner PDFViva IndriyaniAinda não há avaliações
- Nursing Theories and Practice Smith Marlaine C SRG PDFDocumento565 páginasNursing Theories and Practice Smith Marlaine C SRG PDFLerma Delasondra100% (1)
- Customize Heading/Text: Add A Heading HereDocumento2 páginasCustomize Heading/Text: Add A Heading Herehimmatul aliyahAinda não há avaliações
- SMG Clinical Best Practices Print BW NauseaDocumento25 páginasSMG Clinical Best Practices Print BW Nauseahimmatul aliyahAinda não há avaliações
- Nursing Theories and Practice Smith Marlaine C SRG PDFDocumento565 páginasNursing Theories and Practice Smith Marlaine C SRG PDFLerma Delasondra100% (1)
- Nursing Theories and Practice Smith Marlaine C SRG PDFDocumento565 páginasNursing Theories and Practice Smith Marlaine C SRG PDFLerma Delasondra100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Dentinogenesis (AuthorV Mazuru)Documento40 páginasDentinogenesis (AuthorV Mazuru)Octavian DavidsonAinda não há avaliações
- Jaundice Natural RemediesDocumento12 páginasJaundice Natural RemediesprkshshrAinda não há avaliações
- GM Mastery 01Documento53 páginasGM Mastery 01Pa DooleyAinda não há avaliações
- Airway Management 1Documento17 páginasAirway Management 1kamel6Ainda não há avaliações
- Covid 19 Form Excl. Rapid Test - Travel - NamibiaDocumento1 páginaCovid 19 Form Excl. Rapid Test - Travel - NamibiaMa JobsAinda não há avaliações
- PEDOMAN Tatalaksana Cedera Otak 2014Documento96 páginasPEDOMAN Tatalaksana Cedera Otak 2014hasanAinda não há avaliações
- Abnormal Uterine ActionDocumento64 páginasAbnormal Uterine ActionKanimozhi Kasinathan100% (1)
- Problem in Complete Denture Treatment and Postinsertion DentureDocumento35 páginasProblem in Complete Denture Treatment and Postinsertion DentureSorabh JainAinda não há avaliações
- Note GuideDocumento2 páginasNote GuideDemetrius Hobgood0% (1)
- 2017ijmrcr PDFDocumento57 páginas2017ijmrcr PDFIvan InkovAinda não há avaliações
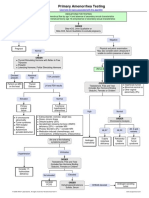
- Primary Amenorrhea Testing AlgorithmDocumento1 páginaPrimary Amenorrhea Testing AlgorithmGabriella AguirreAinda não há avaliações
- Human Performance and Limitations PDFDocumento163 páginasHuman Performance and Limitations PDFJustinAinda não há avaliações
- NeurosyphilisDocumento8 páginasNeurosyphilisl1o2stAinda não há avaliações
- Minnesota State High School LeagueDocumento2 páginasMinnesota State High School Leagueapi-301794844Ainda não há avaliações
- Lecture Notes - BIOS1170B (Body Systems - (Structure and Function) ) (Sydney)Documento86 páginasLecture Notes - BIOS1170B (Body Systems - (Structure and Function) ) (Sydney)SK AuAinda não há avaliações
- Short Stories For KidsDocumento14 páginasShort Stories For KidsSherine Lois QuiambaoAinda não há avaliações
- Effectiveness of Self Myofascial Release On Pain and Functional Ability in Recreational Runners With Medial Tibial Stress SyndromeDocumento3 páginasEffectiveness of Self Myofascial Release On Pain and Functional Ability in Recreational Runners With Medial Tibial Stress SyndromePaulRajAinda não há avaliações
- ECCO 2 Hemodynamics TestDocumento3 páginasECCO 2 Hemodynamics TestpamoralesAinda não há avaliações
- ENGLISH GRAMMER For STD 6Documento21 páginasENGLISH GRAMMER For STD 6Joy OtanielAinda não há avaliações
- Hypotonic Hypertonic Isotonic Solutions UsesDocumento9 páginasHypotonic Hypertonic Isotonic Solutions UsesImtiaz AhmedAinda não há avaliações
- Atlante Immagini PillcamDocumento116 páginasAtlante Immagini PillcamshiprasumanAinda não há avaliações
- Cardiac MonitorDocumento3 páginasCardiac MonitorShameera M. KamlianAinda não há avaliações
- Chest RadiographyDocumento65 páginasChest RadiographyMunish Dogra100% (1)
- Bio P1 SBP 2007Documento23 páginasBio P1 SBP 2007Rozaini Othman100% (2)
- Tutorial Dr. SaugiDocumento33 páginasTutorial Dr. SaugifemmytaniaAinda não há avaliações
- Chapter 4 Tissue - The Living FabricDocumento23 páginasChapter 4 Tissue - The Living FabricMariaAinda não há avaliações
- Chapter 6 ProblemsDocumento2 páginasChapter 6 Problemswalt richardsAinda não há avaliações
- Reminiscences of An Old TimerDocumento524 páginasReminiscences of An Old TimersuneelmadhavAinda não há avaliações
- Full Autopsy Released in Death of Kyler PresnellDocumento9 páginasFull Autopsy Released in Death of Kyler PresnellKrystyna May67% (3)
- D 5 LRDocumento2 páginasD 5 LRDianelie BacenaAinda não há avaliações