Você também pode gostar
- Fluid Environment of the BrainNo EverandFluid Environment of the BrainHelen CserrAinda não há avaliações
- WrightSinclair-CSFandLPpracticalreview 2012JNeuroDocumento19 páginasWrightSinclair-CSFandLPpracticalreview 2012JNeuroIoana CucuAinda não há avaliações
- Cerebellar Ataxia: Pathophysiology and RehabilitationDocumento24 páginasCerebellar Ataxia: Pathophysiology and RehabilitationNistara Singh ChawlaAinda não há avaliações
- Corpus Callosotomy in Children and The Disconnection Syndromes: A ReviewDocumento9 páginasCorpus Callosotomy in Children and The Disconnection Syndromes: A ReviewCraig JohnsonAinda não há avaliações
- AA Issue-Article 9Documento11 páginasAA Issue-Article 9Ethan AmalAinda não há avaliações
- A Brief Overview of The Cerebrospinal Fluid System and Its Implications For Brain and Spinal Cord DiseasesDocumento7 páginasA Brief Overview of The Cerebrospinal Fluid System and Its Implications For Brain and Spinal Cord Diseasesgwyneth.green.512Ainda não há avaliações
- Ocular Blood FlowDocumento451 páginasOcular Blood FlowDwi Atikah SariAinda não há avaliações
- The Delay Phenomenon: A Compilation of Knowledge Across SpecialtiesDocumento7 páginasThe Delay Phenomenon: A Compilation of Knowledge Across SpecialtiesRoger Zambrana FloresAinda não há avaliações
- Research GateDocumento12 páginasResearch GateMae PAinda não há avaliações
- NIH Public Access: Infantile Hydrocephalus: A Review of Epidemiology, Classification and CausesDocumento18 páginasNIH Public Access: Infantile Hydrocephalus: A Review of Epidemiology, Classification and CausesKiki FatmawatyAinda não há avaliações
- Manuscript NeurorehabNeuralRepair Revision4 PublishedVersionDocumento42 páginasManuscript NeurorehabNeuralRepair Revision4 PublishedVersionangelostivencb14Ainda não há avaliações
- Hydrocephalous ModelDocumento18 páginasHydrocephalous Modelpriyadarade97Ainda não há avaliações
- Cerebrospinal Fluid & Blood Brain BarrierDocumento50 páginasCerebrospinal Fluid & Blood Brain BarrierJyothsna DevanadhAinda não há avaliações
- Intravenous Cannula: A Rescue Tool For Cerebrospinal Uid DiversionDocumento3 páginasIntravenous Cannula: A Rescue Tool For Cerebrospinal Uid DiversionChiNdy AfiSaAinda não há avaliações
- Lumbar PunctureDocumento23 páginasLumbar Puncturemamoon100% (2)
- The Human Central Canal of The Spinal Cord A ComprDocumento14 páginasThe Human Central Canal of The Spinal Cord A ComprnaamiiAinda não há avaliações
- s12987 016 0025 2 PDFDocumento20 páginass12987 016 0025 2 PDFNovia AyuAinda não há avaliações
- Nonsurgical Therapy For Hydrocephalus: A Comprêhnsive and Critical ReviewDocumento20 páginasNonsurgical Therapy For Hydrocephalus: A Comprêhnsive and Critical ReviewntnquynhproAinda não há avaliações
- Head Injuries: Yunus Elon, S.Kep., NS., MSN Faculty of Nursing Adventist University of IndonesiaDocumento24 páginasHead Injuries: Yunus Elon, S.Kep., NS., MSN Faculty of Nursing Adventist University of IndonesiachrisamariaAinda não há avaliações
- Electrochemical Failure of The Brain Cortex Is More Deleterious When It Is Accompanied by Low PerfusionDocumento15 páginasElectrochemical Failure of The Brain Cortex Is More Deleterious When It Is Accompanied by Low PerfusionEugenio CapielloAinda não há avaliações
- Human Biology - Respiration - 2023Documento22 páginasHuman Biology - Respiration - 2023eleneking02Ainda não há avaliações
- Neuro Anatomy & Pathophysiology Laboratory Manual - 2 Semester, S. Y 2019 - 2020Documento6 páginasNeuro Anatomy & Pathophysiology Laboratory Manual - 2 Semester, S. Y 2019 - 2020cris baligodAinda não há avaliações
- 1 SM PDFDocumento4 páginas1 SM PDFRika SuryanaAinda não há avaliações
- Peripheral Nerve Repair and Reconstruction PDFDocumento9 páginasPeripheral Nerve Repair and Reconstruction PDFDea Alberta SAinda não há avaliações
- Anatomy of Eyes: January 2009Documento7 páginasAnatomy of Eyes: January 20091710105 Sean Rio SimangunsongAinda não há avaliações
- Extracorporeal Membrane Oxygenation Support in PedDocumento8 páginasExtracorporeal Membrane Oxygenation Support in Pedwalid hassanAinda não há avaliações
- Krishnan2019 Article NeuroimagingInPediatricHydroceDocumento9 páginasKrishnan2019 Article NeuroimagingInPediatricHydroceBrenoAinda não há avaliações
- Abbott2018 Article TheRoleOfBrainBarriersInFluidMDocumento21 páginasAbbott2018 Article TheRoleOfBrainBarriersInFluidMAhmad Al-Husain100% (1)
- Avian Cardiovascular Disease Characteristics, Causes and GenomicsDocumento24 páginasAvian Cardiovascular Disease Characteristics, Causes and GenomicsMonik TanAinda não há avaliações
- ICSE Board Class X Biology Board Paper 2015 (Solution)Documento7 páginasICSE Board Class X Biology Board Paper 2015 (Solution)DAMAYANTI MITRAAinda não há avaliações
- Physiology of CSFDocumento72 páginasPhysiology of CSFtheobudusAinda não há avaliações
- 1430 FullDocumento8 páginas1430 Fullganesh goreAinda não há avaliações
- ThesisDocumento125 páginasThesisNaung Htoo OoAinda não há avaliações
- Cerebrospinal Fluid & Blood Brain Barrier: DR Mohd ImranDocumento50 páginasCerebrospinal Fluid & Blood Brain Barrier: DR Mohd ImranB JYOTHSNAAinda não há avaliações
- Neural Tube DefectDocumento21 páginasNeural Tube Defectmariam bassemAinda não há avaliações
- Paper Draft Revised V3Documento9 páginasPaper Draft Revised V3Berkay CalıskanAinda não há avaliações
- Study Questions Special SensesDocumento37 páginasStudy Questions Special SensesSurajit Bhattacharjee93% (14)
- Fsurg 09 864385Documento10 páginasFsurg 09 864385ja.arenas904pfizerAinda não há avaliações
- Meditation DopamineDocumento6 páginasMeditation DopamineRafael PereiraAinda não há avaliações
- OPTH 143132 Iridocorneal Endothelial Syndrome Clinical PerspectivesDocumento8 páginasOPTH 143132 Iridocorneal Endothelial Syndrome Clinical PerspectivesDr. Abhishek OnkarAinda não há avaliações
- Cerebrospinal FluidDocumento13 páginasCerebrospinal Fluidsakshi panwarAinda não há avaliações
- Diagnostic Challenges in Musculoskeletal Radiology PDFDocumento182 páginasDiagnostic Challenges in Musculoskeletal Radiology PDFphuong mai leAinda não há avaliações
- Endoscopic Transnasal Repair of CSF Rhinorrhea TecDocumento8 páginasEndoscopic Transnasal Repair of CSF Rhinorrhea TecChiNdy AfiSaAinda não há avaliações
- Axelrod Face-selectiveneuronsinthevicinityofthehumanFusiformFaceAreaDocumento17 páginasAxelrod Face-selectiveneuronsinthevicinityofthehumanFusiformFaceAreaNico NicoAinda não há avaliações
- CSF LeaksDocumento11 páginasCSF Leakssudheer joelAinda não há avaliações
- Cerebrospinal Fluid Its StructureDocumento1 páginaCerebrospinal Fluid Its StructurePraneeth KumarAinda não há avaliações
- Metaanális de Los Factores de Riesgo en La Enfermedad de ParkinsonDocumento8 páginasMetaanális de Los Factores de Riesgo en La Enfermedad de ParkinsonAlejandraTiradoAinda não há avaliações
- +++ 4 мозкова рболонкаDocumento7 páginas+++ 4 мозкова рболонкаIryna ZapekaAinda não há avaliações
- Case Report Embolic Shotgun Pellet To The Righ 2024 International JournalDocumento5 páginasCase Report Embolic Shotgun Pellet To The Righ 2024 International JournalRonald QuezadaAinda não há avaliações
- CPC IndicationsDocumento5 páginasCPC IndicationsCarlos Daniel Giménez MéndezAinda não há avaliações
- Journal Reading: Fakultas Kedokteran Universitas Islam Sultan Agung SemarangDocumento20 páginasJournal Reading: Fakultas Kedokteran Universitas Islam Sultan Agung SemaranghetidwiputriAinda não há avaliações
- Veenstra 2013Documento5 páginasVeenstra 2013Rafael CostaAinda não há avaliações
- Meningitis, Encphalitis, NeurocystecercosisDocumento91 páginasMeningitis, Encphalitis, NeurocystecercosisjialeongAinda não há avaliações
- Free Radicals and Neuronal Recovery From An IschaeDocumento18 páginasFree Radicals and Neuronal Recovery From An IschaeMarcos SánchezAinda não há avaliações
- NiedeckcirculDocumento8 páginasNiedeckcirculRe̸ina pla̸ysAinda não há avaliações
- Reconstruction of The Face and Neck With Different Types of Pre-Expanded Anterior Chest Aps: A Comprehensive Strategy For Multiple TechniquesDocumento9 páginasReconstruction of The Face and Neck With Different Types of Pre-Expanded Anterior Chest Aps: A Comprehensive Strategy For Multiple TechniquesMohd Rehan QureshiAinda não há avaliações
- Polytrauma NewDocumento69 páginasPolytrauma NewdrsyedabdhahirAinda não há avaliações
- Extracorporeal Membrane Oxygenation in Critically Ill ChildrenDocumento16 páginasExtracorporeal Membrane Oxygenation in Critically Ill ChildrenEduardo Rios DuboisAinda não há avaliações
- Dor de Cabeça CervicalDocumento16 páginasDor de Cabeça CervicalCleômenes NetoAinda não há avaliações
- Lecture 13 - Capillary Circulation, Edema FormationDocumento24 páginasLecture 13 - Capillary Circulation, Edema Formationmurtada gubaAinda não há avaliações
- 922 FullDocumento7 páginas922 FullCharina Geofhany DeboraAinda não há avaliações
- Comparison of The Effects of Clobazam and Diazepam in Prevention of Recurrent Febrile SeizuresDocumento2 páginasComparison of The Effects of Clobazam and Diazepam in Prevention of Recurrent Febrile SeizuresCharina Geofhany DeboraAinda não há avaliações
- Comparison of The Effects of Clobazam and Diazepam in Prevention of Recurrent Febrile Seizures PDFDocumento5 páginasComparison of The Effects of Clobazam and Diazepam in Prevention of Recurrent Febrile Seizures PDFCharina Geofhany DeboraAinda não há avaliações
- Acute Surgical Abdomen: An Unusual Presentation of Pulmonary EmbolusDocumento4 páginasAcute Surgical Abdomen: An Unusual Presentation of Pulmonary EmbolusCharina Geofhany DeboraAinda não há avaliações
- Acute Cerebral Infarction Masked by A Brain Tumor: Kwo-Whei Lee Chung-Ping LoDocumento6 páginasAcute Cerebral Infarction Masked by A Brain Tumor: Kwo-Whei Lee Chung-Ping LoCharina Geofhany DeboraAinda não há avaliações
- Grade 7 CH 4.05 The HeartDocumento12 páginasGrade 7 CH 4.05 The HeartMunmun AfnanAinda não há avaliações
- HorribleWounds PosterDocumento1 páginaHorribleWounds PosterNfikf100% (1)
- Fracturi de Coloana Cervicala, Toracala Si LombaraDocumento770 páginasFracturi de Coloana Cervicala, Toracala Si Lombaracomir2002100% (3)
- 1st BDS Oral Histology and Dental AnotomyDocumento11 páginas1st BDS Oral Histology and Dental AnotomyAmrutha Dasari100% (1)
- Difference Between Primary and Permanent TeethDocumento15 páginasDifference Between Primary and Permanent TeetharthisaAinda não há avaliações
- Exercise 19 Serial Transverse Section of A 48 Hour Chick Embryo PDFDocumento11 páginasExercise 19 Serial Transverse Section of A 48 Hour Chick Embryo PDFMichaela FayeAinda não há avaliações
- Technical Dictionary of DancingDocumento62 páginasTechnical Dictionary of DancingRory CorbettAinda não há avaliações
- 84359Documento5 páginas84359Pedro Gouveia100% (1)
- Blue Boxes Lower LimbDocumento4 páginasBlue Boxes Lower LimbZllison Mae Teodoro MangabatAinda não há avaliações
- 3 Bagua Internal Warm-Up MethodDocumento65 páginas3 Bagua Internal Warm-Up Methodvincraig100% (2)
- Quick Review - Fossa of RosenmullerDocumento4 páginasQuick Review - Fossa of RosenmullerDavis KallanAinda não há avaliações
- DXA PRIMUSم الصادقDocumento3 páginasDXA PRIMUSم الصادقBahaa Aldeen FadhilAinda não há avaliações
- Effectiveness of Deep Pharyngeal Neuromuscular Stimulation Versus Thermal Gustatory Stimulation in Decreasing Length of Swallow Initiation and Improving Lingual Movements - Maria H WillisDocumento54 páginasEffectiveness of Deep Pharyngeal Neuromuscular Stimulation Versus Thermal Gustatory Stimulation in Decreasing Length of Swallow Initiation and Improving Lingual Movements - Maria H WillisconstantineeliaAinda não há avaliações
- Skeletal System PowerpointDocumento40 páginasSkeletal System PowerpointLee KaiYangAinda não há avaliações
- Overview of Cardiovascular System: An Introduction To Chapters 9 - 24 and Chapter 36 Guyton and Hall, 12 EditionDocumento10 páginasOverview of Cardiovascular System: An Introduction To Chapters 9 - 24 and Chapter 36 Guyton and Hall, 12 EditionbahahahahAinda não há avaliações
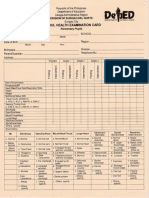
- School Health Examination Card For ElementaryDocumento2 páginasSchool Health Examination Card For ElementaryWilma Villanueva86% (21)
- HypothyroidismDocumento43 páginasHypothyroidismRama Krishnan100% (2)
- Part of Body & Istilah Medis KeperawatanDocumento61 páginasPart of Body & Istilah Medis KeperawatanFholsen FrohansenAinda não há avaliações
- The Far-Lateral Approach and Its Transcondylar, Supracondylar, and Paracondylar ExtensionsDocumento15 páginasThe Far-Lateral Approach and Its Transcondylar, Supracondylar, and Paracondylar Extensionsbodeadumitru9261Ainda não há avaliações
- Cardiac Conduction System - Normal Function of The Heart - Cardiology Teaching Package - Practice Learning - Division of Nursing - The University of NottinghamDocumento3 páginasCardiac Conduction System - Normal Function of The Heart - Cardiology Teaching Package - Practice Learning - Division of Nursing - The University of Nottinghamlilsmiddy0% (1)
- JACK HEGGIE e Moshe FeldenkraisDocumento77 páginasJACK HEGGIE e Moshe FeldenkraisAdriana M. VillalónAinda não há avaliações
- Muscles of The Lower Limb (ADAM)Documento18 páginasMuscles of The Lower Limb (ADAM)محمد علىAinda não há avaliações
- Locomotor Homoeopathy PDFDocumento80 páginasLocomotor Homoeopathy PDFmartincorbacho100% (1)
- Weekly AssignmentDocumento7 páginasWeekly AssignmentBajwa AyeshaAinda não há avaliações
- Madbarz Routines Plan: Strength - AdvancedDocumento18 páginasMadbarz Routines Plan: Strength - AdvancedJuan Sebastian AnguloAinda não há avaliações
- Basic Position Where Most Exercises BeginDocumento9 páginasBasic Position Where Most Exercises BeginAgik ParAinda não há avaliações
- Baza III Curs MedDocumento117 páginasBaza III Curs MedIntekhabAtahar0% (1)
- Plexopathy and MononeuropathyDocumento38 páginasPlexopathy and MononeuropathySOUMYADEEP BHUINYAAinda não há avaliações
- Pemeriksaan AbdomenDocumento212 páginasPemeriksaan Abdomentamara hanna bocanAinda não há avaliações
- QuestionsDocumento3 páginasQuestionsshone123Ainda não há avaliações