Você também pode gostar
- Interactions With Experimental COVID-19 Therapies: Please Check For UpdatesDocumento27 páginasInteractions With Experimental COVID-19 Therapies: Please Check For UpdatesMayra caplaAinda não há avaliações
- Hemo Obstetrica PDFDocumento10 páginasHemo Obstetrica PDFMayra caplaAinda não há avaliações
- Articulo 2 AnestesioDocumento7 páginasArticulo 2 AnestesioMayra caplaAinda não há avaliações
- Clinical Practice Guidelines For Colon Volvulus and Acute Colonic Pseudo-ObstructionDocumento12 páginasClinical Practice Guidelines For Colon Volvulus and Acute Colonic Pseudo-ObstructionMayra caplaAinda não há avaliações
- Anestesio Dental PDFDocumento7 páginasAnestesio Dental PDFMayra caplaAinda não há avaliações
- Autophagy in Lysosomal MyopathiesDocumento7 páginasAutophagy in Lysosomal MyopathiesMayra caplaAinda não há avaliações
- Microbiology 2004 0211Documento12 páginasMicrobiology 2004 0211Mayra caplaAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Aew 312Documento14 páginasAew 312ZulfajriAinda não há avaliações
- 45a6 Arterial en PerrosDocumento12 páginas45a6 Arterial en Perrosandres silvaAinda não há avaliações
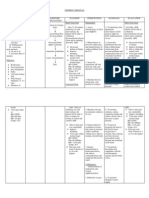
- NURSING CARE PLAN For Myocardial InfarctionDocumento13 páginasNURSING CARE PLAN For Myocardial Infarctionbanyenye2593% (14)
- Sport and Exercise Physiology: Questions 650-655Documento14 páginasSport and Exercise Physiology: Questions 650-655Bach XuanAinda não há avaliações
- Pulmonary HipertensionDocumento481 páginasPulmonary HipertensionFransiskus A Danu KrisbiantoroAinda não há avaliações
- Mindray BeneView T8Documento2 páginasMindray BeneView T8irwin kurniadiAinda não há avaliações
- Levels of Care Intensive Care Society 2009Documento14 páginasLevels of Care Intensive Care Society 2009bogus987Ainda não há avaliações
- Physiological Adaptation of Cardiovascular System To High AltitudeDocumento11 páginasPhysiological Adaptation of Cardiovascular System To High AltitudeNicholas Matthew SantosoAinda não há avaliações
- Anesthesia For The Pet Practitioner (Banfield, 2003 Edition) PDFDocumento125 páginasAnesthesia For The Pet Practitioner (Banfield, 2003 Edition) PDFB.L.C.SAinda não há avaliações
- HDO Leaflet PTDocumento12 páginasHDO Leaflet PTErickson Fabian CastilloAinda não há avaliações
- Decreased Cardiac OutputDocumento5 páginasDecreased Cardiac Outputshuang81Ainda não há avaliações
- Test Bank Chapter 67: Nursing Management: Shock, Systemic Inflammatory Response Syndrome, and Multiple Organ Dysfunction SyndromeDocumento11 páginasTest Bank Chapter 67: Nursing Management: Shock, Systemic Inflammatory Response Syndrome, and Multiple Organ Dysfunction Syndromebbianca1990100% (1)
- Integrated Cardiovascular Physiology: A Laboratory ExerciseDocumento70 páginasIntegrated Cardiovascular Physiology: A Laboratory ExercisefireworkrwAinda não há avaliações
- 1985-Cardiac Adaptations To Chronic ExerciseDocumento28 páginas1985-Cardiac Adaptations To Chronic ExerciseJavier Mora BaizAinda não há avaliações
- MasterScreen-CPX BR EN PDFDocumento2 páginasMasterScreen-CPX BR EN PDFLajoskaAinda não há avaliações
- Skills Checklist: CARESCAPE™ Monitor B850Documento14 páginasSkills Checklist: CARESCAPE™ Monitor B850Jonathan ScottAinda não há avaliações
- Ewquickguide 2 EdDocumento188 páginasEwquickguide 2 EdStanley Wu TaiAinda não há avaliações
- BTL CardioPoint-CPET CLIN ClinicalBackground EN100Documento26 páginasBTL CardioPoint-CPET CLIN ClinicalBackground EN100stoicea catalinAinda não há avaliações
- Quiz___Answers_Combined.pdfDocumento25 páginasQuiz___Answers_Combined.pdfzuimaoAinda não há avaliações
- Impaired Swallowing: Nursing Care PlanDocumento6 páginasImpaired Swallowing: Nursing Care PlanEloidaValdezZuluetaAinda não há avaliações
- Ecocardiografia NeonatalDocumento10 páginasEcocardiografia NeonatalRonald MHAinda não há avaliações
- DNB QUESTION PAPER-Topic Wise (Author DR - Sirisha)Documento92 páginasDNB QUESTION PAPER-Topic Wise (Author DR - Sirisha)Sirisha CkvAinda não há avaliações
- Flow Chart For Pinsky-Vincent Protocol: Intensive Care UnitDocumento5 páginasFlow Chart For Pinsky-Vincent Protocol: Intensive Care UnitRaditya Indah TofaniAinda não há avaliações
- Perinatology Clinics 2008, Vol.35, Issues 4, Neuroprotection in The NewbornDocumento210 páginasPerinatology Clinics 2008, Vol.35, Issues 4, Neuroprotection in The NewbornJhonny MarquezAinda não há avaliações
- Ea (Dyn)Documento9 páginasEa (Dyn)Dr.Biswajit jenaAinda não há avaliações
- B105 Patient Monitor: Care With ConfidenceDocumento5 páginasB105 Patient Monitor: Care With ConfidenceNoe Muñoz QuitoAinda não há avaliações
- Hypertension NCPDocumento4 páginasHypertension NCPChristian Karl B. Llanes0% (2)
- Capnography & Multigas: Supplies & AccessoriesDocumento25 páginasCapnography & Multigas: Supplies & AccessoriesfugarisaAinda não há avaliações
- Clinical Exercise TestingDocumento339 páginasClinical Exercise TestingandreianklAinda não há avaliações
- Flotrac Algorithm White PaperDocumento4 páginasFlotrac Algorithm White PaperAnestesia 2017 UDECAinda não há avaliações