Você também pode gostar
- Fascial Manipulation Practical Part PDFDocumento2 páginasFascial Manipulation Practical Part PDFBrandi0% (1)
- Study of Pre Analytical Errors in A Medium Sized Pathology LaboratoryDocumento6 páginasStudy of Pre Analytical Errors in A Medium Sized Pathology Laboratorysandeep raiAinda não há avaliações
- Take Ten' Improving The Surgical Post-Take Ward Round A Quality Improvement ProjectDocumento5 páginasTake Ten' Improving The Surgical Post-Take Ward Round A Quality Improvement ProjectJeff ThomasAinda não há avaliações
- 2022 - Educational Nursing Intervention in Reducing Hospital Readmission A Systematic ReviewDocumento15 páginas2022 - Educational Nursing Intervention in Reducing Hospital Readmission A Systematic ReviewArthurAinda não há avaliações
- Concordance With Phase One Cardiac Rehabilitation Guidelines in The Inpatient SettingDocumento7 páginasConcordance With Phase One Cardiac Rehabilitation Guidelines in The Inpatient Settingferi sulistyaAinda não há avaliações
- 1 s2.0 S1386505622002489 MainDocumento8 páginas1 s2.0 S1386505622002489 MainAnayat KhanAinda não há avaliações
- 57 FullDocumento6 páginas57 Full30. Tyanna Putri MinartiAinda não há avaliações
- OhnsDocumento7 páginasOhnsDaniel AbomaAinda não há avaliações
- The REALAB Project A New Method For The PDFDocumento9 páginasThe REALAB Project A New Method For The PDFAdrianaManouAinda não há avaliações
- Using Lean Principles To Optimise Inpatient Phlebotomy ServicesDocumento7 páginasUsing Lean Principles To Optimise Inpatient Phlebotomy ServicesMuizzuddin MuizAinda não há avaliações
- Nursing Practice Today: Behrouz Pakcheshm, Imane Bagheri Zohreh KalaniDocumento9 páginasNursing Practice Today: Behrouz Pakcheshm, Imane Bagheri Zohreh KalaniFernando PintoAinda não há avaliações
- RetroDocumento6 páginasRetroMariaAinda não há avaliações
- ADocumento6 páginasAsinnanancyAinda não há avaliações
- Shift Report ProjectDocumento1 páginaShift Report Projectapi-347777703Ainda não há avaliações
- Training Using Simulation in Internal Medicine Residencies: An Educational PerspectiveDocumento3 páginasTraining Using Simulation in Internal Medicine Residencies: An Educational PerspectiveagaetioAinda não há avaliações
- 1 s2.0 S1553725021000982 MainDocumento7 páginas1 s2.0 S1553725021000982 MainNovia khasanahAinda não há avaliações
- Jurnal Pendukung PDFDocumento12 páginasJurnal Pendukung PDFMita AmaliaAinda não há avaliações
- Medical Staff Satisfaction Survey in A Makeshift Emergency Pandemic Covid Hospital - September - 2022 - 2012312667 - 4023723Documento3 páginasMedical Staff Satisfaction Survey in A Makeshift Emergency Pandemic Covid Hospital - September - 2022 - 2012312667 - 4023723sanjay yadavAinda não há avaliações
- Fluid Administration For Acute Circulatory Dysfunction Using Basic Monitoring Narrative Review and Expert Panel Recommendations From An ESICM Task Force Maurizio CecconDocumento12 páginasFluid Administration For Acute Circulatory Dysfunction Using Basic Monitoring Narrative Review and Expert Panel Recommendations From An ESICM Task Force Maurizio CecconEllys Macías PeraltaAinda não há avaliações
- A Framework For Evaluating The Appropriateness of Clinical Decision Support Alerts and ResponsesDocumento8 páginasA Framework For Evaluating The Appropriateness of Clinical Decision Support Alerts and ResponsesSocorro Moreno LunaAinda não há avaliações
- Escala de Agotamiento - Recuperación Ocupacional PDFDocumento6 páginasEscala de Agotamiento - Recuperación Ocupacional PDFJorge Gabriel Chan CoobAinda não há avaliações
- Indirect Methods For Reference Interval Determination - Review and RecommendationsDocumento10 páginasIndirect Methods For Reference Interval Determination - Review and RecommendationsDuy HoangAinda não há avaliações
- 3 Minute Diabetic Foot ExamDocumento8 páginas3 Minute Diabetic Foot ExamLorrieAinda não há avaliações
- EBP Practice 3 - C - JackDischarge09Documento11 páginasEBP Practice 3 - C - JackDischarge09Sitti Rosdiana YahyaAinda não há avaliações
- Hex 21 41Documento16 páginasHex 21 41fadedoyinAinda não há avaliações
- Pengantar Ilmu Fiqih IslamDocumento10 páginasPengantar Ilmu Fiqih IslamHI DayatAinda não há avaliações
- Jones Etal 2019 Enhanced SupervisionDocumento10 páginasJones Etal 2019 Enhanced SupervisionErick TavaresAinda não há avaliações
- Establishing Reference Intervals For Clinical Laboratory Test Results (2010)Documento7 páginasEstablishing Reference Intervals For Clinical Laboratory Test Results (2010)Duy HoangAinda não há avaliações
- 5.1 Hand Hygiene Intervention Efficacy ComparisonDocumento14 páginas5.1 Hand Hygiene Intervention Efficacy ComparisonQworldAinda não há avaliações
- Schoch 2014Documento35 páginasSchoch 2014Bianca CorreiaAinda não há avaliações
- Recognition of Clinical Deterioration, A Clinical Leadership Opportunity For Nurse ExecutiveDocumento6 páginasRecognition of Clinical Deterioration, A Clinical Leadership Opportunity For Nurse ExecutivePAULA SORAIA CHENAinda não há avaliações
- Nursing A 2Documento9 páginasNursing A 2nehayayayaseenAinda não há avaliações
- Development and Validation of PACICDocumento9 páginasDevelopment and Validation of PACICKristen LynchAinda não há avaliações
- REACT Rapid Evaluation Assessment of Clinical ReasoningRoolDocumento6 páginasREACT Rapid Evaluation Assessment of Clinical ReasoningRoolFrederico PóvoaAinda não há avaliações
- The Effectiveness of Primary Care Streaming in Emergency D - 2022 - InternationaDocumento7 páginasThe Effectiveness of Primary Care Streaming in Emergency D - 2022 - InternationaTheerapat Chalerm-MuangAinda não há avaliações
- Reeder 2003Documento6 páginasReeder 2003Nurul AidaAinda não há avaliações
- ArticleDocumento5 páginasArticleJay StoneAinda não há avaliações
- Scoping Review of Pediatric Early Warning SystemsDocumento29 páginasScoping Review of Pediatric Early Warning SystemsCantika SRAinda não há avaliações
- Depuccio 2020Documento8 páginasDepuccio 2020Rita RangelAinda não há avaliações
- JCDR 8 FC05Documento4 páginasJCDR 8 FC05Mohammed AdemAinda não há avaliações
- Adherence of Physicians Practice Tonational Ministry of Health (Moh) Urgent Care Guideline in Eastern Region, Saudi ArabiaDocumento9 páginasAdherence of Physicians Practice Tonational Ministry of Health (Moh) Urgent Care Guideline in Eastern Region, Saudi ArabiaIJAR JOURNALAinda não há avaliações
- Adherence of Physicians Practice Tonational Ministry of Health (Moh) Urgent Care Guideline in Eastern Region, Saudi ArabiaDocumento9 páginasAdherence of Physicians Practice Tonational Ministry of Health (Moh) Urgent Care Guideline in Eastern Region, Saudi ArabiaIJAR JOURNALAinda não há avaliações
- Operational Ef Ficiency and Productivity Improvement Initiatives in A Large Cardiac Catheterization LaboratoryDocumento10 páginasOperational Ef Ficiency and Productivity Improvement Initiatives in A Large Cardiac Catheterization LaboratorySajad HayatAinda não há avaliações
- Case Study Discretion Advised PDFDocumento12 páginasCase Study Discretion Advised PDFGustavo MooriAinda não há avaliações
- Ghosh 2021Documento6 páginasGhosh 2021Yonatan MeshaAinda não há avaliações
- Journal of Clinical Nursing - 2022 - Burke - Factors That Influence Hospital Nurses Escalation of Patient Care in ResponseDocumento50 páginasJournal of Clinical Nursing - 2022 - Burke - Factors That Influence Hospital Nurses Escalation of Patient Care in ResponsePaulaAinda não há avaliações
- Hospital Management SystemDocumento6 páginasHospital Management SystemYohannes KefyalewAinda não há avaliações
- Healthcare 2Documento8 páginasHealthcare 2Noor KhanAinda não há avaliações
- Impacts of An Acute Care Telenursing Program On Discharge, Patient Experience, and Nursing Experience: Retrospective Cohort Comparison StudyDocumento10 páginasImpacts of An Acute Care Telenursing Program On Discharge, Patient Experience, and Nursing Experience: Retrospective Cohort Comparison Studylismuc.pa.21Ainda não há avaliações
- Journal Homepage: - : IntroductionDocumento9 páginasJournal Homepage: - : IntroductionIJAR JOURNALAinda não há avaliações
- The Effect of Structured Teaching Program On Knowledge About Arterial Blood Gas Analysis Among The Staff Nurses Working in Critical Care UnitDocumento7 páginasThe Effect of Structured Teaching Program On Knowledge About Arterial Blood Gas Analysis Among The Staff Nurses Working in Critical Care UnitIJAR JOURNALAinda não há avaliações
- Improving Patient Care Outcomes Through Better Delegation-Communication Between Nurses and Assistive PersonnelDocumento7 páginasImproving Patient Care Outcomes Through Better Delegation-Communication Between Nurses and Assistive PersonneltasyaAinda não há avaliações
- Artikel Ebsco 3Documento7 páginasArtikel Ebsco 3bakena bajentaAinda não há avaliações
- Introduction:-: Journal HomepageDocumento6 páginasIntroduction:-: Journal HomepageIJAR JOURNALAinda não há avaliações
- Quality Indicators, Performance Measures, and Accountability: The Right Thing, at The Right Time, For The Right ReasonDocumento8 páginasQuality Indicators, Performance Measures, and Accountability: The Right Thing, at The Right Time, For The Right ReasonMulyawan Safwandy NugrahaAinda não há avaliações
- Health Expectations - 2017 - Rojas García - Impact and Experiences of Delayed Discharge A Mixed Studies Systematic ReviewDocumento16 páginasHealth Expectations - 2017 - Rojas García - Impact and Experiences of Delayed Discharge A Mixed Studies Systematic ReviewGabriela ObonAinda não há avaliações
- A Review of The Evidence and Recommendations On Communication Skills and The PatientDocumento26 páginasA Review of The Evidence and Recommendations On Communication Skills and The PatientThayna MirandaAinda não há avaliações
- 4 AeeDocumento6 páginas4 AeeAlberto Jr. AndresAinda não há avaliações
- Activity-Based Costing of Health-Care Delivery, Haiti: ResearchDocumento8 páginasActivity-Based Costing of Health-Care Delivery, Haiti: ResearchFelixpro DotaAinda não há avaliações
- Applying Lean Principles To Reduce Wait Times in A VA Emergency DepartmentDocumento10 páginasApplying Lean Principles To Reduce Wait Times in A VA Emergency DepartmentNida KhoiriahAinda não há avaliações
- The Maximally Efficient and Optimally Effective Emergency Department: One Good Thing A DayNo EverandThe Maximally Efficient and Optimally Effective Emergency Department: One Good Thing A DayAinda não há avaliações
- Central Venous Catheters: Iv Terapy &Documento71 páginasCentral Venous Catheters: Iv Terapy &Florence Liem0% (1)
- Olympus BF Channels-DesinfDocumento1 páginaOlympus BF Channels-DesinfEduardo ArreguinAinda não há avaliações
- Aubf Quiz 2Documento8 páginasAubf Quiz 2Gene Narune GaronitaAinda não há avaliações
- Prenatal DevelopmentDocumento29 páginasPrenatal DevelopmentReymart MancaoAinda não há avaliações
- Precautionary and Sanitary Practices in Handling FoodDocumento31 páginasPrecautionary and Sanitary Practices in Handling FoodBrenNan ChannelAinda não há avaliações
- tmpD1AB TMPDocumento9 páginastmpD1AB TMPFrontiersAinda não há avaliações
- Chronic Obstructive Pulmonary DiseaseDocumento36 páginasChronic Obstructive Pulmonary DiseaseHazel ManuelAinda não há avaliações
- Perbedaan Kadar Hbsag Sampel Serum Dan Plasma Metode Clia Pada PendonorDocumento7 páginasPerbedaan Kadar Hbsag Sampel Serum Dan Plasma Metode Clia Pada PendonorAAK DHGRiski MaulanaAinda não há avaliações
- IVD Medical Device V2Documento44 páginasIVD Medical Device V2Vadi VelanAinda não há avaliações
- Diabetic FootDocumento47 páginasDiabetic FootadhikarisamirAinda não há avaliações
- Oplan Kalusugan Sa DepEd SY 2019Documento4 páginasOplan Kalusugan Sa DepEd SY 2019Klaribelle Villaceran100% (1)
- Hemophilia: Factor IX (Hemophilia B)Documento38 páginasHemophilia: Factor IX (Hemophilia B)Jhvhjgj JhhgtyAinda não há avaliações
- Lefort FractureDocumento90 páginasLefort FractureRiya CorreaAinda não há avaliações
- Emergency Nursing Nclex ExamDocumento19 páginasEmergency Nursing Nclex ExamsjardioAinda não há avaliações
- NTU Cat Management Network Annual General Report For Academic Year 2016/2017Documento42 páginasNTU Cat Management Network Annual General Report For Academic Year 2016/2017Cat Management NetworkAinda não há avaliações
- Introduction To Homoeopathic PharmacyDocumento12 páginasIntroduction To Homoeopathic PharmacyPreethika PadmanabanAinda não há avaliações
- Sepsis en El Embarazo y PuerperioDocumento9 páginasSepsis en El Embarazo y PuerperioJoseTeodomiroQuispeRicciAinda não há avaliações
- 2nd Grading Test Science 5Documento7 páginas2nd Grading Test Science 5LeonorBagnisonAinda não há avaliações
- Points From Accupuncture AtlasDocumento1 páginaPoints From Accupuncture AtlasdishkuAinda não há avaliações
- The 100 Most Influential Publications in Paracetamol Poisoning TreatmentDocumento81 páginasThe 100 Most Influential Publications in Paracetamol Poisoning TreatmentPetrov MihaelaAinda não há avaliações
- Worksheet For Nervous Systems-KeyDocumento5 páginasWorksheet For Nervous Systems-KeyNazarine Torres100% (2)
- List of Instruments For 2nd Year BDSDocumento17 páginasList of Instruments For 2nd Year BDSMohammad ShoebAinda não há avaliações
- ChoreaDocumento4 páginasChoreaapi-19973386Ainda não há avaliações
- ACETYLCYSTEINEDocumento2 páginasACETYLCYSTEINEAubrey Unique EvangelistaAinda não há avaliações
- Post Natal ExercisesDocumento7 páginasPost Natal ExercisesEvie Dolpin BlueAinda não há avaliações
- Health and Nutrition in Islam: Ideas, Just New People To Discover Them." It Is, in Fact, Amazing ToDocumento2 páginasHealth and Nutrition in Islam: Ideas, Just New People To Discover Them." It Is, in Fact, Amazing ToWakhyulianto MobeeAinda não há avaliações
- DiphtheriaDocumento11 páginasDiphtheriabrigde_xAinda não há avaliações
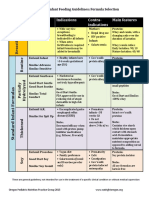
- Formula Selection OPNPGDocumento2 páginasFormula Selection OPNPGRina PratiwiAinda não há avaliações
- Magnesium Nitrate HexahydrateDocumento4 páginasMagnesium Nitrate HexahydrateCarmen M AvinazarAinda não há avaliações